Chapter: Paediatrics: Paediatric Surgery
Paediatrics: Midgut malrotation and volvulus
Midgut malrotation and volvulus
During the first trimester of
intrauterine development the foetal midgut transiently herniates into the
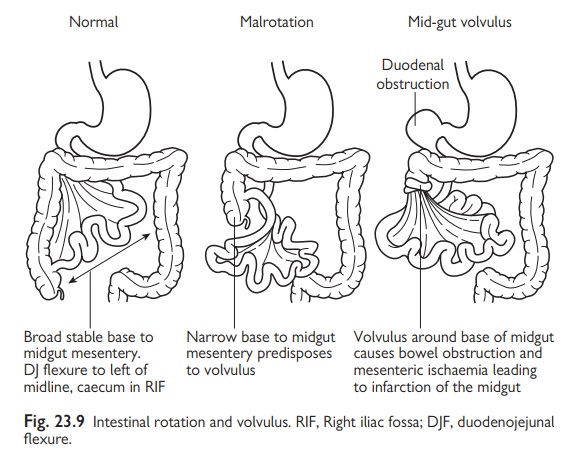
umbilical cord. As this reduces, the mesentery normally rotates to bring the
cae-cum to lie in the right iliac fossa and duodenojejunal flexure (DJF) to lie
to the left of the midline. The midgut mesentery thus extends diagonally across
the back of the abdominal cavity and provides a broad stable pedi-cle for the
SMA to supply the bowel. Malrotation is a failure of this normal rotation that
leaves the caecum high in the right upper quadrant and DJF mobile in midline.
The result is a narrow base for the midgut mesentery and a narrow mobile
pedicle through which the SMA runs. Malrotation is usually asymptomatic and
only detected by contrast meal and follow through.
Midgut malrotation
•
Midgut
malrotation predisposes to midgut volvulus.
•
To
prevent this complication, surgical correction of a malrotation is advised
using Ladd’s procedure.
•
An
incidental appendicectomy is usually performed.
Midgut volvulus
•
This
is a catastrophic event that occurs without warning.
· The immediate effect is high
intestinal obstruction at duodenal level that is rapidly followed by infarction
of the entire midgut.
Symptoms
•
Bile-stained
vomiting.
•
Circulatory
collapse.
•
Tender
abdomen.
Diagnosis
•
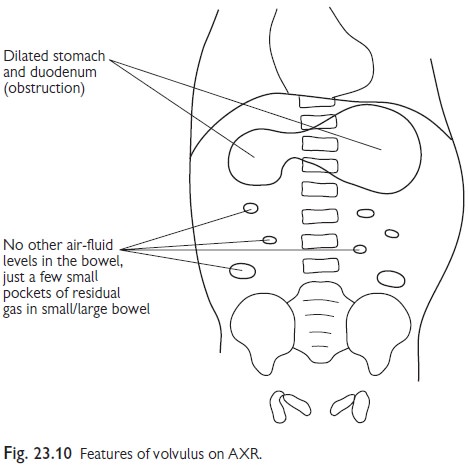
AXR
(Fig. 23.10). May appear similar to duodenal atresia with a ‘double bubble’ and
a paucity of gas elsewhere in the abdomen.
•
The
diagnosis is confirmed by an urgent (even middle of the night) upper GI
contrast study.
Surgical treatment
•
Immediate
laparotomy to untwist the volvulus.
•
If the
bowel is healthy a Ladd’s procedure is performed.
If bowel viability is doubtful a second look laparotomy may be necessary after 24hr. Frequently, there is massive intestinal necrosis and the child is left with a very short gut in which case long-term IV feeding is required.
Related Topics