Chapter: Case Study in Obstetrics and Gynaecology: Emergency Gynaecology
Case Study Reports: Abdominal Pain
ABDOMINAL PAIN
History
A
14-year-old girl presents
with lower abdominal
pain which developed
suddenly a day ago.
The pain is over the whole lower
abdomen but worse
on the right. It was intermittent
at first but is now constant and very severe.
She feels unwell in herself
with no appetite and vomiting. She now feels sweaty as well.
She says her bowels opened normally
the day before and they are normally regular.
She
has never had any previous
episode of pain like this.
Her last menstrual period started 2 weeks
ago and she
has a slightly irregular cycle.
She has never
had any gynaecological or other medical problems
in the past.
Examination
On
examination she looks
in pain and seems to find it difficult to get comfortable. Her tem- perature is
37.9°C, pulse 112/min and blood
pressure 116/74 mmHg. She feels warm and well
perfused. The abdomen
is distended symmetrically with generalized tenderness, max- imal in the right iliac
fossa region. There
is rebound and guarding in the right
iliac fossa.
Questions
·
What is the differential diagnosis?
·
How
would you investigate and manage this girl?
Answer:
The differential diagnosis of right
iliac fossa pain in this case is:
gynaecological:
·
adnexal/ovarian cyst torsion
·
ovarian cyst rupture
·
ovarian cyst haemorrhage
·
ectopic pregnancy
surgical:
·
appendicitis
urinary:
·
urinary tract infection
·
renal colic
The
girl is acutely
systemically unwell with an acute
abdomen which would
favour the diagnosis of torsion or possibly ruptured
appendix. Cyst rupture
and haemorrhage are not
commonly associated with such systemic
disturbance, though this is an important differ- ential diagnosis.
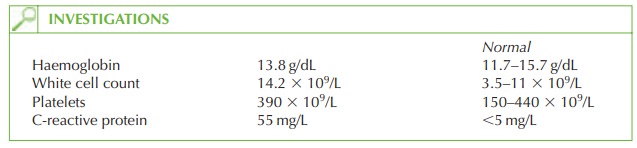
Further investigation would include
a pregnancy test to exclude
pregnancy, and urinaly- sis to exclude urinary
tract infection or renal colic. An ultrasound should be arranged (transabdominal) to assess for an ovarian
cyst or for an inflamed
appendix. If an adnexal
mass is confirmed, laparoscopy or laparotomy should be performed
as soon as possible since adnexal
torsion is associated with loss of the ovarian
function if ischaemia
is pro- longed and necrosis occurs.
Ovarian torsion can often be managed by detorsion, though oophorectomy sometimes may be necessary.
If
the diagnosis is not clear between appendicitis and ovarian torsion
then joint lapar- otomy or laparoscopy with
the surgical team
is an appropriate approach.
Related Topics