Chapter: Case Study in Obstetrics and Gynaecology: Emergency Gynaecology
Case Study Reports: Abdominal Pain and Vaginal Discharge
ABDOMINAL PAIN AND VAGINAL DISCHARGE
History
A
46-year-old Indian woman
presents with a month-long history
of increasing abdom- inal pain and a green/yellow vaginal
discharge. For the last few days she had been feel-
ing feverish and unwell. The pain is across the lower abdomen
but worse on the left.
She has no urinary
symptoms and has
been opening her
bowels normally. She
has a reduced appetite and mild nausea but has not vomited.
She
has had two vaginal deliveries in the past and no other pregnancies. She had a lapar-
otomy about 4 years ago for drainage
of a pelvic abscess. Recently
she has been under the care
of a gynaecologist for heavy
and prolonged periods,
for which she is taking
cyclical norethisterone. There is no other
medical or surgical
history of note.
Examination
The temperature is 37.8°C, pulse
95/min and blood pressure is 136/76 mmHg. The abdomen appears slightly distended and a mass
is palpated arising
from the pelvis
on the left. There
is focal tenderness in the left iliac fossa
without rebound tenderness or guard- ing. Speculum
examination reveals no discharge or blood, and the cervix
appears normal. Cervical excitation and bilateral adnexal
tenderness are noted,
more marked on the left.
Questions
·
What is the differential diagnosis?
·
Why is she anaemic?
·
How
would you further
investi- gate and manage
this patient?
Answer:
The
woman is acutely
unwell with pyrexia,
tachycardia, raised inflammatory markers, neutrophilia and reactive
thrombocythaemia. This suggests
an infective process
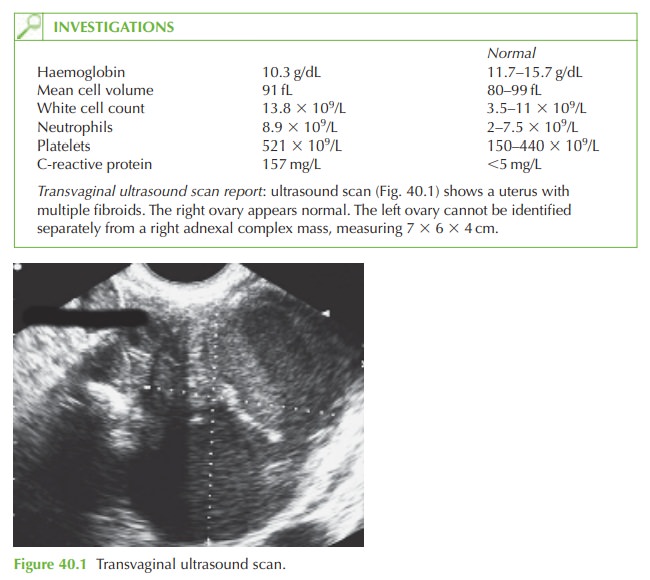
and the left iliac
fossa mass detected
on ultrasound would
appear to be the cause.
The likely diag- nosis is a tubo-ovarian mass, probably an abscess.
Alternatively this could potentially be a diverticular abscess or, if it were on the right,
an appendix abscess. Ovarian malignancy or another cause of a complex
adnexal mass would be unlikely
to present with this acute inflammatory episode.
Anaemia in this woman
could be due to chronic
menorrhagia or anaemia
of chronic dis- ease. The increased mean cell volume
suggests the latter,
but ferritin and folate levels would be useful to see whether
there is in fact a degree of iron deficiency too.
Further investigations
Blood cultures and vaginal
and endocervical swabs should be taken. Ferritin
and folate should be checked.
Management
The woman should be admitted for
intravenous antibiotics. Broad-spectrum cover should be given including agents
against anaerobes and
chlamydia. In cases
of pelvic inflamma- tory disease (PID) there
is commonly a mixed growth
of anaerobes on top of a previous chlamydial infection. If improvement does not occur within 24–48 h, or the diagnosis
is unclear, then laparoscopy or laparotomy should be performed
to confirm the diagnosis
and drain the abscess surgically.
Related Topics