Chapter: Medicine and surgery: Nervous system
Trigeminal nerve (V) lesion - Disorders of cranial nerves
Trigeminal nerve (V) lesion
Anatomy
Emerges as two roots (large sensory and small motor root), passes out forwards the pons into the posterior cranial fossa and across the temporal lobe in the middle cranial fossa. The nerve expands to form the trigeminal ganglion, at the petrous temporal bone, and gives off 3 branches: ophthalmic (V1), maxillary (V2) and mandibular (V3).
Function
The motor components supply the muscles of mastication and tensor tympani.
The sensory components supply the sensation of the face:
i. V1 supplies the forehead, the upper eyelid and eyeball.
ii. V2 supplies the lower eyelid, the side of the nose, the upper teeth and the upper lip.
iii. V3 supplies the mandible, the ear and the skin and
mucous membranes of the lower jaw.
Pain and temperature fibres are also carried on the three divisions back to the trigeminal ganglion, but then dive down into the medulla to the spinal nucleus of V which extends as far as the upper cervical cord.
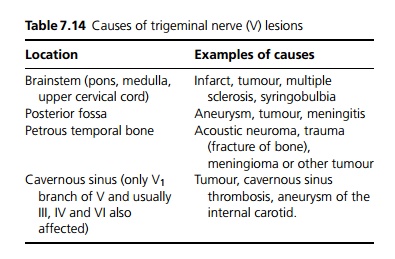
Specific causes
Causes are shown in Table 7.14. Herpes zoster can infect the trigeminal nerve.
Clinical features
Sensory: Complete loss of sensation on one side of the face – if all branches are affected the lesion must be at the level of the ganglion or above. The earliest sign is loss of the corneal reflex. Dissociated sensory loss (i.e. loss of pain but touch intact) suggests only the spinal nucleus is affected, e.g. by syringobulbia or a foramen magnum tumour. If touch is lost, but pain and temperature intact, the lesion has to be in the pons or medulla.
Motor: When the mouth is opened, the lower jaw deviates to the side of the lesion.
Related Topics