Chapter: Basic & Clinical Pharmacology : Management of the Poisoned Patient
Toxic Syndromes: Antidepressants
ANTIDEPRESSANTS
Tricyclic antidepressants (eg, amitriptyline, desipramine, doxe-pin, many others;) are among the most common prescription drugs involved in life-threatening drug overdose. Ingestion of more than 1 g of a tricyclic (or about 15–20 mg/kg) is considered potentially lethal.
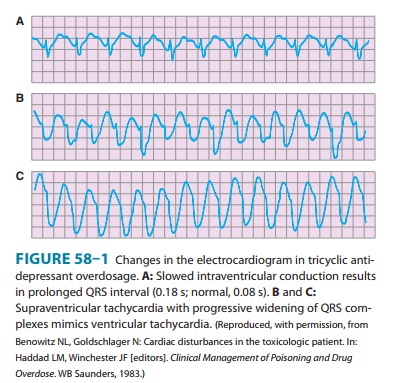
Tricyclic antidepressants are competitive antagonists at musca-rinic cholinergic receptors, and anticholinergic findings (tachycar-dia, dilated pupils, dry mouth) are common even at moderate doses. Some tricyclics are also strong α blockers, which can lead to vasodilation. Centrally mediated agitation and seizures may be followed by depression and hypotension. Most important is the fact that tricyclics have quinidine-like cardiac depressant effects on the sodium channel that cause slowed conduction with a wide QRS interval and depressed cardiac contractility. This cardiactoxicity may result in serious arrhythmias (Figure 58–1), including ventricular conduction block and ventricular tachycardia.
Treatment of tricyclic antidepressant overdose includes general supportive care as outlined earlier. Endotracheal intubation and assisted ventilation may be needed. Intravenous fluids are given for hypotension, and dopamine or norepinephrine is added if necessary. Many toxicologists recommend norepinephrine as the initial drug of choice for tricyclic-induced hypotension. The anti-dote for quinidine-like cardiac toxicity (manifested by a wide QRS complex) is sodium bicarbonate: a bolus of 50–100 mEq (or 1–2 mEq/kg) provides a rapid increase in extracellular sodium that helps overcome sodium channel blockade. Do not use physo-stigmine! Although this agent does effectively reverse anticholin-ergic symptoms, it can aggravate depression of cardiac conduction and cause seizures.
Monoamine oxidase inhibitors (eg, tranylcypromine, phenel-zine) are older antidepressants that are occasionally used for resis-tant depression. They can cause severe hypertensive reactions when interacting foods or drugs are taken, and they can interact with the selective serotonin reuptake inhibi-tors (SSRIs).
Newer antidepressants (eg, fluoxetine, paroxetine, citalopram,venlafaxine) are mostly SSRIs and are generally safer than the tri-cyclic antidepressants and monoamine oxidase inhibitors, although they can cause seizures. Bupropion (not an SSRI) has caused sei-zures even in therapeutic doses. Some antidepressants have been associated with QT prolongation and torsades de pointes arrhyth-mia. SSRIs may interact with each other or especially with mono-amine oxidase inhibitors to cause the serotonin syndrome, characterized by agitation, muscle hyperactivity, and hyperthermia .
Related Topics