Chapter: Essentials of Anatomy and Physiology: An Introduction to Microbiology and Human Disease
The Pathogens and its List
THE PATHOGENS
In the sections that follow, each group of pathogens will be described with a summary of important char-acteristics. Examples of specific pathogens will be given to help you become familiar with them. Tables
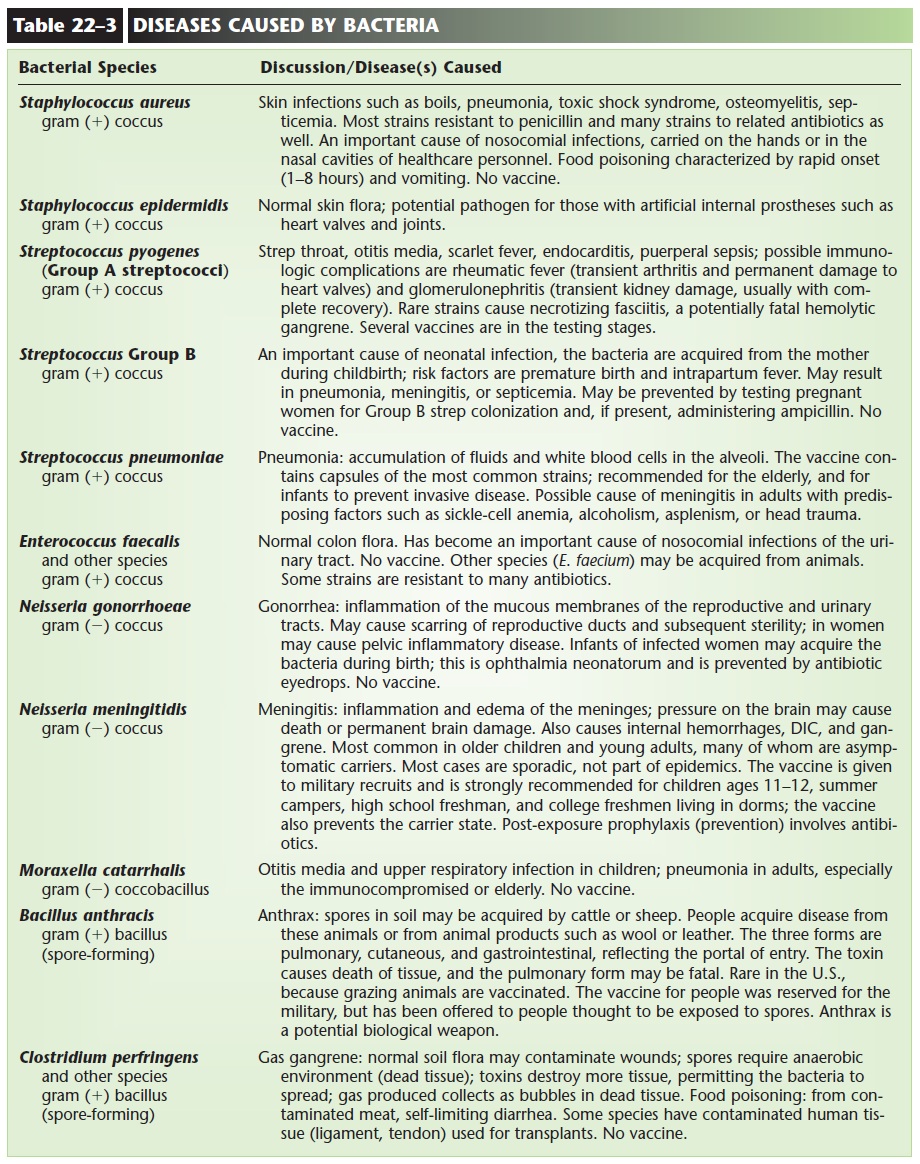
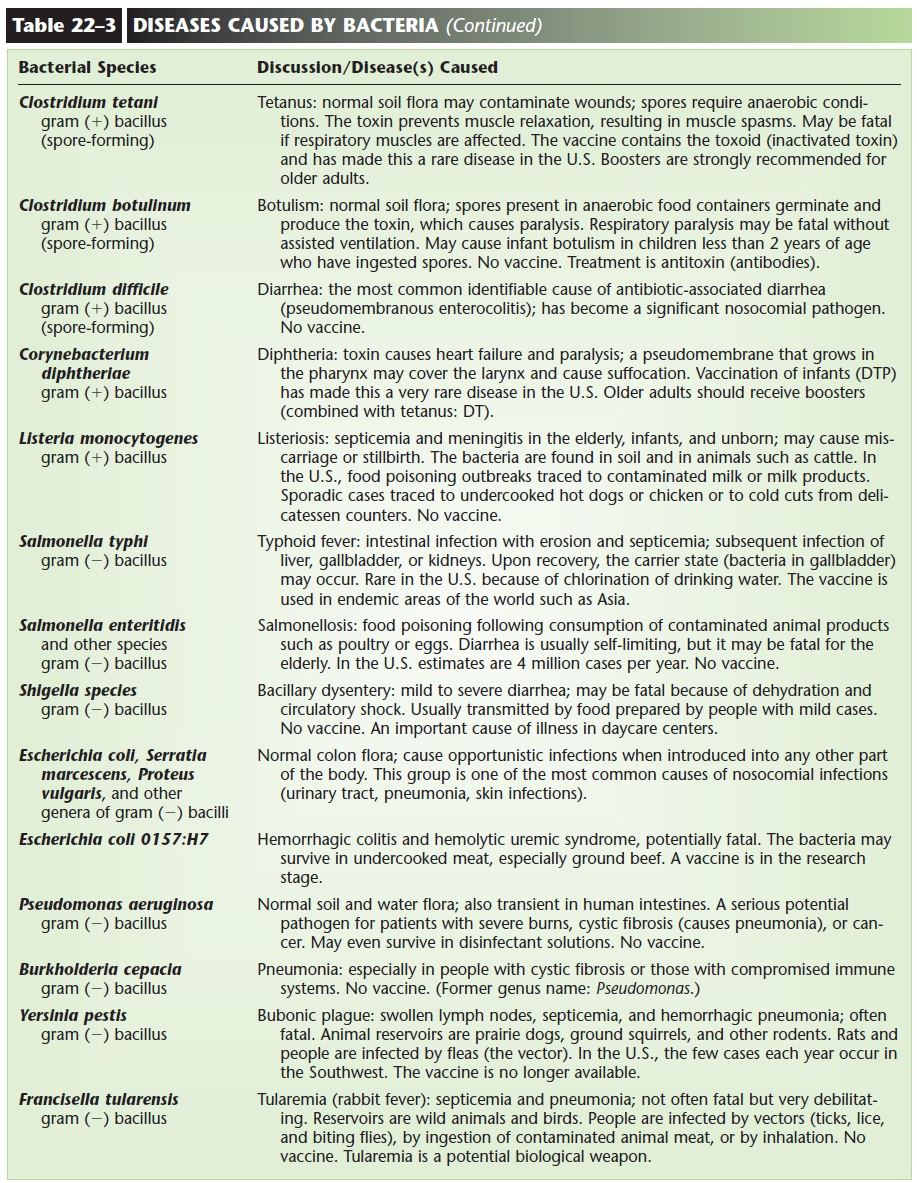
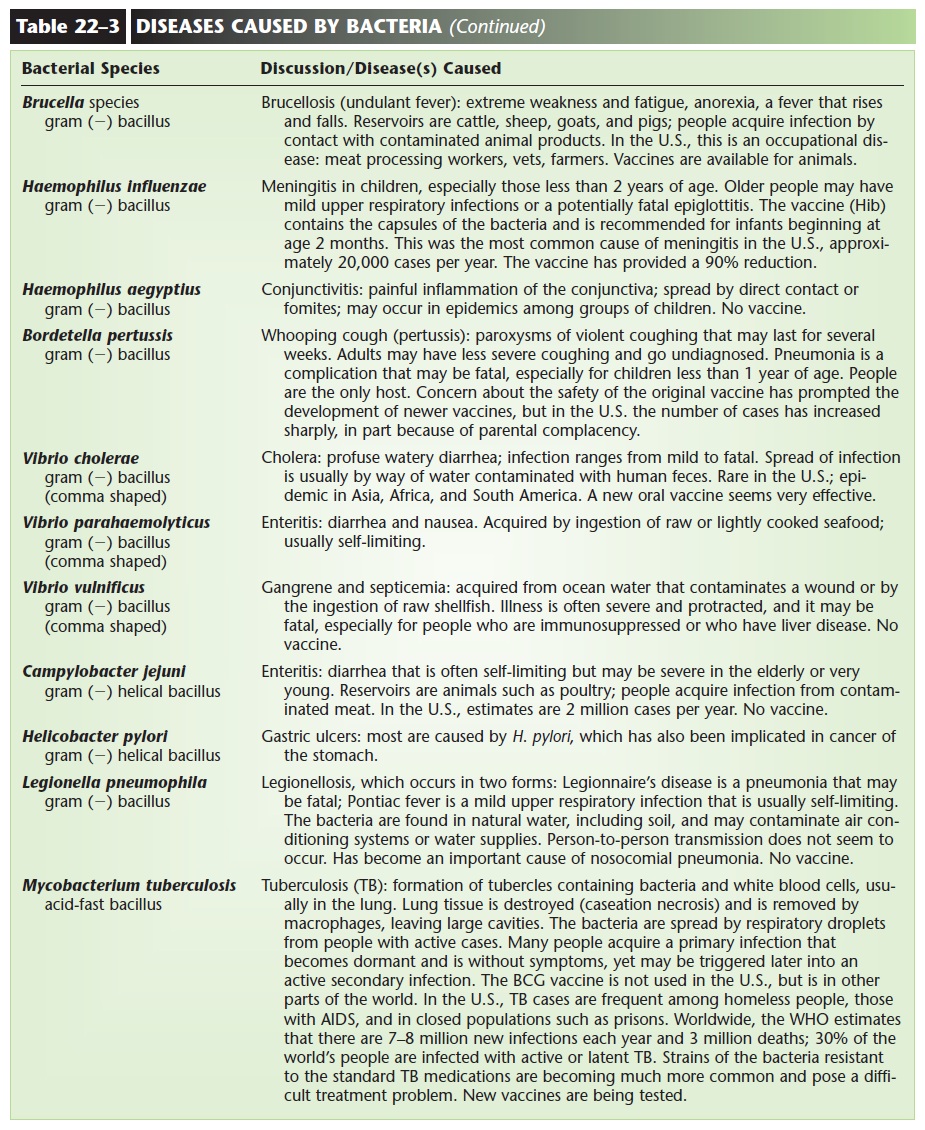
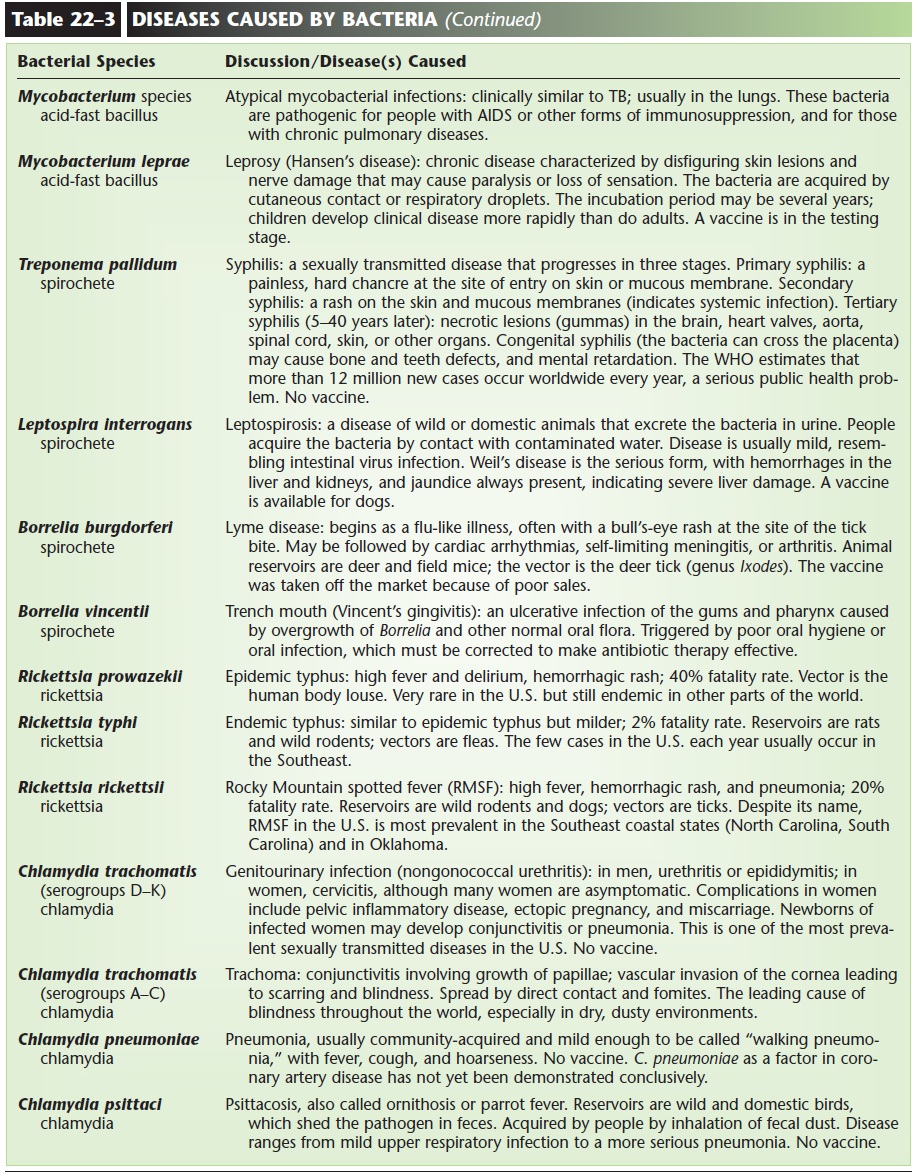
BACTERIA (SEE TABLE 22–3)
Bacteria are very simple unicellular organisms. All are microscopic in size, and a magnification of 1000 times is usually necessary to see them clearly. A bacterial cell consists of watery cytoplasm and a single chromosome (made of DNA) surrounded by a cell membrane. Enclosing all of these structures is a cell wall, which is strong and often rigid, giving the bacterium its char-acteristic shape.
Based on shape, bacteria are classified as one of three groups: coccus, bacillus, or spirillum (Fig. 22–2). A coccus (plural: cocci) is a sphere; under the micro-scope, cocci appear round. Certain prefixes may be used to describe the arrangement of spheres. Staphylomeans clusters, strepto refers to chains of cells, and diplo means pairs of cells.
A bacillus (plural: bacilli) is a rod-shaped bac-terium; rods may vary in length depending on the genus. A spirillum (plural: spirilla) is a long cell with one or more curves or coils. Some spirilla, such as those that cause syphilis and Lyme disease, are calledspirochetes. Many of the bacilli and spirilla are capa-ble of movement because they have flagella. These are long, thread-like structures that project from the cell and beat rhythmically.
Bacteria reproduce by the process of binary fis-sion, in which the chromosome duplicates itself, and the original cell divides into two identical cells. The presence or absence of oxygen may be important for bacterial reproduction. Aerobic bacteria can repro-duce only in the presence of oxygen, and anaerobic bacteria can reproduce only in the absence of oxygen. Facultatively anaerobic bacteria are not inhibited in either situation; they are able to reproduce in either the presence or absence of oxygen. This is obviously an advantage for the bacteria, and many pathogens and potential pathogens are facultative anaerobes.
The Gram Stain
Based on the chemicals in their cell walls, most bacte-ria can be put into one of two groups, called gram positive or gram negative. A simple laboratory pro-cedure called the Gram stain (see Fig. 22–2) shows us the shape of the bacteria and their gram reactions. Gram-positive bacteria appear purple or blue, and gram-negative bacteria appear pink or red. Some bac-teria do not stain with the Gram method (many spir- illa and spirochetes do not), but for those that do, each genus is either gram positive or gram negative. This does not change, just as the characteristic shape of the bacteria does not change. The genus Streptococcus, for example, is always a gram-positive coccus; the genus Escherichia is always a gram-negative bacillus. If a Gram stain is done on a sputum specimen from a patient with pneumonia, and a gram-positive coccus is found, this eliminates all of the gram-negative cocci and bacilli that may also cause pneumonia. The Gram stain, therefore, is often an important first step in the identification of the pathogen that is causing a partic-ular infection. In Table 22–3 (at the end of this chap-ter), the gram reaction (where applicable) and shape are included for each pathogen.
Special Characteristics
Although bacteria are simple cells, many have special structural or functional characteristics that help them to survive. Some bacilli and cocci have capsules (see Fig. 22–2); a capsule is a gelatinous sheath that enclo-ses the entire cell. Capsules are beneficial to the bac-teria because they inhibit phagocytosis by the host’s white blood cells. This gives the bacteria time to reproduce and possibly establish themselves in the host. This is not beneficial from our point of view (remember that we are the hosts), but bacterial cap-sules are also antigenic, which means that they stim-ulate antibody production by our lymphocytes. This starts the destruction of bacteria by our immune responses. We take advantage of this by using bacter-ial capsules in some of our vaccines, such as those used to prevent pneumonia and meningitis.
Some bacilli are able to survive unfavorable envi-ronments by forming spores. A spore is a dormant (inactive) stage that consists of the chromosome and a small amount of cytoplasm surrounded by a thick wall. Spores can survive conditions such as heat (even boil-ing), freezing, or dehydration, which would kill the vegetative (active) forms of the bacterial cells. Fortunately for us, most pathogens are unable to form spores, but some that do are the causative agents of gas gangrene, botulism, tetanus, and anthrax. These bac-teria are decomposers in the soil environment, and their spore-forming ability enables them to survive the extremes of temperature and lack of water that may occur in the soil.
Many bacteria cause disease because they produce toxins, which are chemicals that are harmful to host tissues. Often these toxins are the equivalent of our
Some bacterial toxins such as hemolysins and pro-teases literally digest host tissues such as red blood cells and proteins. The bacteria then absorb the digested nutrients.
The toxins of other bacteria have very specific effects on certain cells of the host. Botulism and tetanus toxins, for example, areneurotoxins that disrupt the functioning of nerve cells, leading to the characteristic symptoms of each disease. The diph-theria toxin causes heart failure, the pertussis (whoop-ing cough) toxin immobilizes the cilia of the respiratory tract, and the cholera enterotoxin causes diarrhea.
The cell walls of gram-negative bacteria are made of chemicals called endotoxins. Endotoxins all have the same effects on the host: They cause fever and cir-culatory shock (low blood pressure and heart failure).
Endotoxin shock (also called gram-negative shock) is a life-threatening condition that may accompany any serious infection with gram-negative bacteria.
Rickettsias and Chlamydias
These two groups of bacteria differ from most other bacteria in that they are obligate intracellular para-sites. This means that they can reproduce only within the living cells of a host.
The rickettsias (also: rickettsiae) are parasites of mammals (including people) and are often spread by arthropod vectors. In the United States, the most common rickettsial disease is Rocky Mountain spotted fever, which is spread by ticks. In other parts of the world, epidemic typhus, which is spread by body lice, is still an important disease. From a historical per-spective, until World War I, more people died of epi-demic typhus during times of war than were killed by weapons.
The chlamydias (also: chlamydiae) cause several human diseases, including ornithosis (parrot fever) and trachoma, which is the leading cause of blindness throughout the world. In the United States, chlamy-dial infection of the genitourinary tract has become one of the most prevalent sexually transmitted dis-eases, with estimates of 4 million new cases each year.
Both rickettsial and chlamydial infections can be treated with antibiotics.
Antibiotics
Antibiotics are chemicals that are used to treat bacter-ial infections. A broad-spectrum antibiotic is one that affects many different kinds of bacteria; a narrow-spectrum antibiotic affects just a few kinds of bacteria.
The use of antibiotics is based on a very simple principle: Certain chemicals can disrupt or inhibit the chemical reactions that bacteria must carry out to sur-vive. An antibiotic such as penicillin blocks the forma-tion of bacterial cell walls; without their cell walls, bacteria will die. Other antibiotics inhibit DNA syn-thesis or protein synthesis. These are vital activities for the bacteria, and without them bacteria cannot reproduce and will die.
It is very important to remember that our own cells carry out chemical reactions that are very similar to some of those found in bacteria. For this reason, our own cells may be damaged by antibiotics. This is why some antibiotics have harmful side effects. The most serious side effects are liver and kidney damage or depression of the red bone marrow. The liver is responsible for detoxifying the medication, which may accumulate and damage liver cells. Similar damage may occur in the kidneys, which are responsible for excreting the medication. The red bone marrow is a very active tissue, with constant mitosis and protein synthesis to produce RBCs, WBCs, and platelets. Any antibiotic that interferes with these processes may decrease production of all of these blood cells. Patients who are receiving any of the potentially toxic
antibiotics should be monitored with periodic tests of liver and kidney function or with blood counts to assess the state of the red bone marrow.
Another problem with the use of antibiotics is that bacteria may become resistant to them, and so be unaffected. Bacterial resistancemeans that the bacte-ria are able to produce an enzyme that destroys the antibiotic, rendering it useless. This is a genetic capa-bility on the part of bacteria, and it is, therefore, passed to new generations of bacterial cells.
Let us use an example with small numbers and say that, of 1000 bacterial cells, 998 are killed by a certain antibiotic. The remaining two bacteria have the gene for an enzyme that breaks the antibiotic molecule, so they survive. What will these two bacteria do? Each will divide by binary fission, becoming two cells, four cells, eight cells, and so on. At the end of 20 divisions (which under optimum conditions may take less than 24 hours) each bacterium has become more than a million bacteria. And what is true of all of these bacte-ria? They all have the gene for resistance to that par-ticular antibiotic.
This is exactly what has happened with Staphylo-coccus aureus, most strains of which are resistant to penicillin, and some strains of which are resistant to many other antibiotics as well. Most of the gram-negative intestinal bacilli are resistant to a great vari-ety of antibiotics. This is why culture and sensitivity testing is so important before an antibiotic is chosen to treat these infections.
Education is also important, and healthcare person-nel must help educate the general public not to demand antibiotics for colds or the flu. These are viral diseases for which antibiotics are useless. What hap-pens is that the antibiotic kills all susceptible bacteria (even beneficial ones) and leaves resistant bacteria to become the most numerous, perhaps to cause serious disease in the future.
To counteract bacterial resistance, new antibiotics are produced that are not inactivated by the destruc-tive bacterial enzymes. Within a few years, however, the usefulness of these new antibiotics will probably diminish as bacteria mutate and develop resistance. This is not a battle that we can ever truly win, because bacteria are living organisms that evolve as their envi-ronment changes. We must never underestimate the ability of bacteria to evolve ways to neutralize the antibiotics we use to kill them. The development of new antibiotics is crucial if we are to stay a step ahead of these remarkably adaptable microorganisms.
Antibiotics have changed our lives, although we may not always realize that. A child’s strep throat will probably not progress to meningitis, and bacterial pneumonia does not have the very high fatality rate that it once did. But, we must keep in mind that antibi-otics are not a “cure” for any disease. An infection, especially a serious one, means that the immune sys-tem has been overwhelmed by the pathogen. An antibiotic diminishes the number of bacteria to a level with which the immune system can cope. Ultimately, however, the body’s own white blood cells must elim-inate the very last of the bacteria.
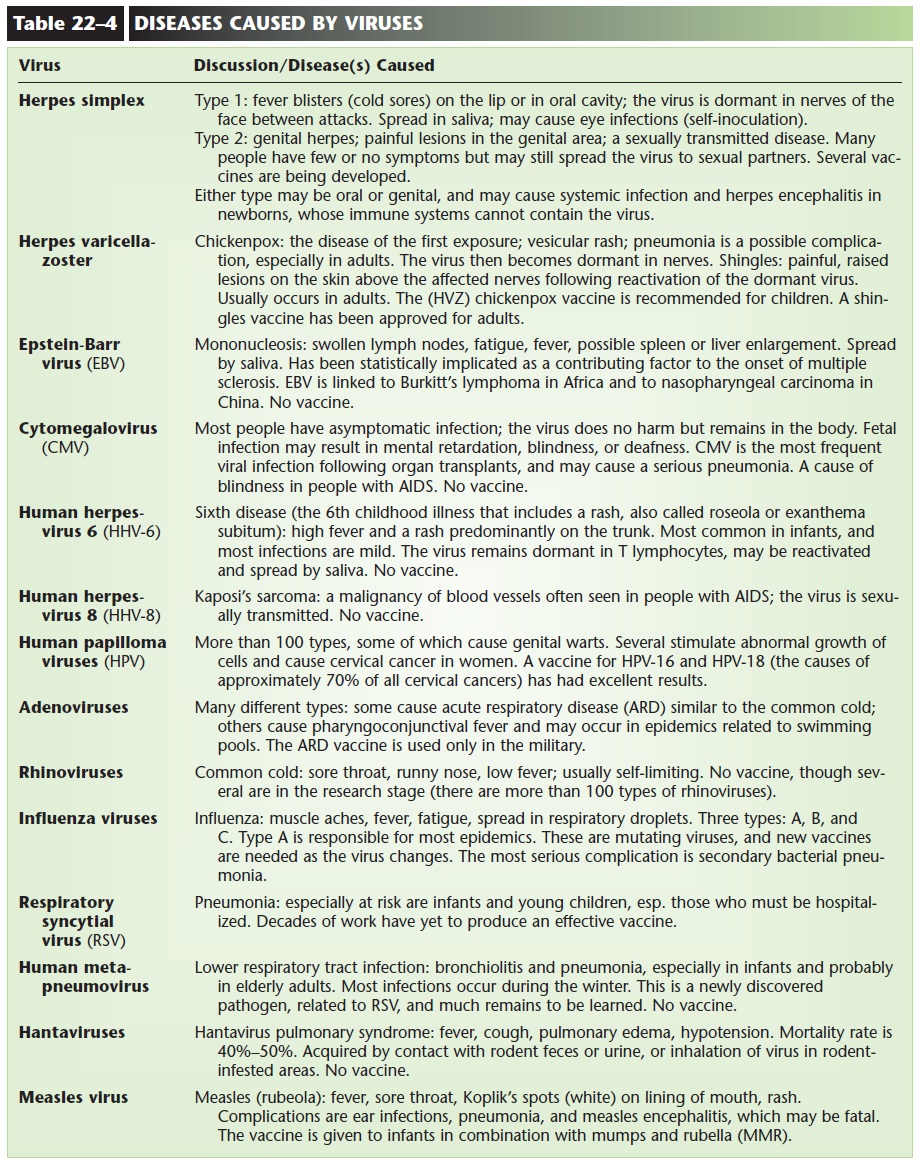
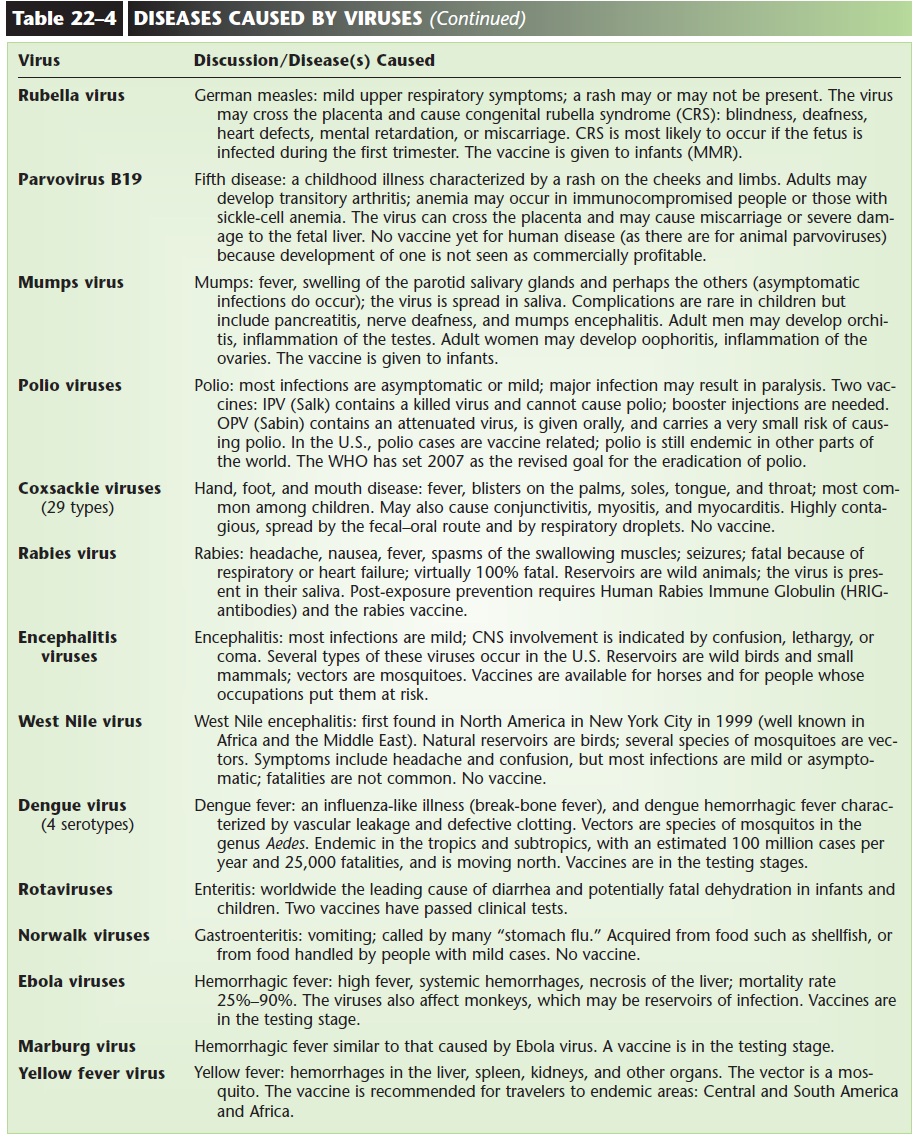
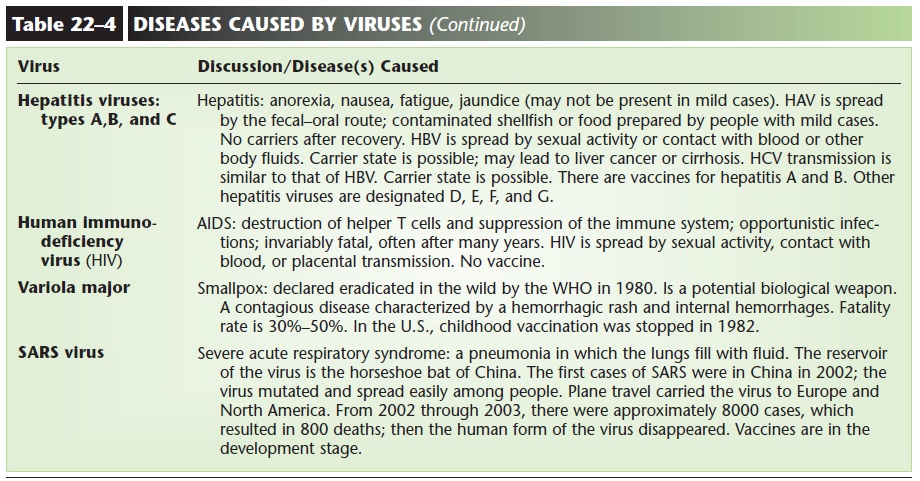
VIRUSES (SEE TABLE 22–4)
Viruses are not cells; their structure is even simpler than that of bacteria, which are the simplest cells. A virus consists of either DNA or RNA surrounded by a protein shell. The protein shell has a shape that is characteristic for each virus (Fig. 22–3). There are no enzymes, cytoplasm, cell membranes, or cell walls in viruses, and they can reproduce only when inside the living cells of a host. Therefore, all viruses are obligate intracellular parasites, and they cause disease when they reproduce inside cells. When a virus enters a host cell, it uses the cell’s chromosomes, RNA, and enzymes to make new viruses. Several hundred new viruses may be produced from just one virus. The host cell rup-tures and dies, releasing the new viruses, which then enter other cells and reproduce.
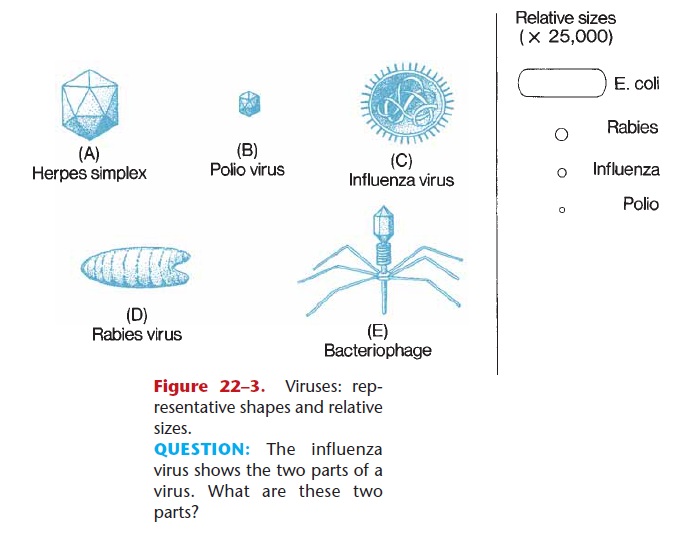
Figure 22–3. Viruses: rep-resentative shapes and relative sizes.
QUESTION: The influenza virus shows the two parts of a virus. What are these two parts?
The severity of a viral disease depends upon the types of cells infected. If the virus affects skin cells, for example, the disease is usually mild and self-limiting, such as chickenpox. Small numbers of skin cells are not crucial to our survival, and these cells can be replaced by mitosis. If, however, the virus affects nerve cells, the disease is more serious and may be fatal. Rabies is such as disease. Neurons are much more vital to us, and they cannot be replaced once they die.
Some viruses, such as those that cause German measles (rubella) and chickenpox, are able to cross the placenta, that is, pass from maternal circulation to fetal circulation. Although the disease may be very mild for the pregnant woman, the virus may severely damage developing fetal organs and cause congenital birth defects such as blindness, heart malformations, and mental retardation. In the most serious cases, fetal infection may result in miscarriage or stillbirth.
Some viruses cause an initial infection, become dormant, then are reactivated, causing another infec-tion months or years later. The herpes viruses that cause cold sores “hide out” in nerves of the face fol-lowing the initial skin lesion. At some later time when the host’s resistance is lowered, the viruses emerge from the nerves and cause another cold sore. The chickenpox virus, which most of us acquire as chil-dren, is a herpes virus that may become dormant in nerves for years, and then be reactivated and cause shingles when we are adults.
A few human viruses are known to be tumor viruses, that is, they cause cells to develop abnormally and form tumors. The Epstein-Barr virus, which causes mononucleosis in North America, is associated with Burkitt’s lymphoma in Africa and with nasopha-ryngeal carcinoma in China. There are environmental factors, as yet unknown, that contribute to the devel-opment of these cancers in specific parts of the world.
Several of the human papillomaviruses have also been associated with cancers of the mouth or larynx, and three of these viruses are found in 90% of cervical car-cinomas in women.
Important viral diseases are described in Table 22–4.
Antiviral Medications
The treatment of viral diseases with chemicals poses some formidable challenges. First, viruses are active (reproducing) only within cells, so the medication must be able to enter infected cells to be effective. Second, viruses are such simple structures that the choice of which of their chemical processes to attempt to disrupt is limited. Third, viruses use the host cell’s DNA and enzymes for self-replication, and a medica-tion that interferes with DNA or enzymes may kill the host cell even as it kills the virus.
These problems are illustrated by zidovudine (AZT), the first medication that was effective against HIV, the virus that causes AIDS. Zidovudine works by interfering with DNA synthesis, which the virus must carry out to reproduce. The side effects of zidovudine, which are experienced by a significant number of AIDS patients, are caused by the disruption of DNA synthesis in the person’s own cells.
Despite these obstacles, successful antiviral drugs have been developed. Acyclovir, for example, has proved to be useful in the control (not cure) of herpes viruses. Ribavirin has been quite effective in the treat-ment of respiratory syncytial virus pneumonia in infants and young children. This is an area of intensive research, and more antiviral medications will undoubtedly be found within the next decade.
We must be aware, however, that many viruses undergo mutations with great frequency. Influenza viruses do (this is the reason we need a new flu vaccine every year), and it was perhaps inevitable that flu virus mutations would provide them with resistance to antiviral medications. In January 2006 the CDC advised physicians not to prescribe amantadine and rimantadine for patients with influenza, because more than 90% of the strains of influenza A virus had devel-oped resistance to both drugs. Staying one step ahead of such viruses may prove to be difficult.
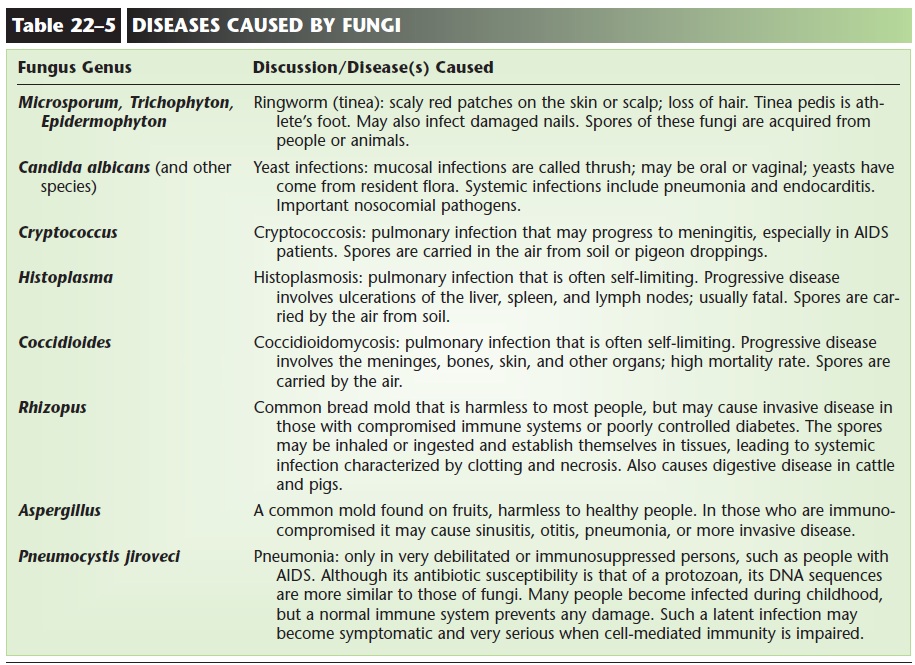
FUNGI (SEE TABLE 22–5)
Fungi may be unicellular, such as yeasts, or multicel-lular, such as the familiar molds and mushrooms. Most fungi are saprophytes(also called saprobes); that is,
they live on dead organic matter and decompose it to recycle the chemicals as nutrients. The pathogenic fungi cause infections that are called mycoses (singu-lar: mycosis), which may be superficial or systemic.
Yeasts (Fig. 22–4) have been used by people for thousands of years in baking and brewing. In small numbers, yeasts such as Candida albicans are part of the resident flora of the skin, mouth, intestines, and vagina. In larger numbers, however, yeasts may cause superficial infections of mucous membranes or the skin, or very serious systemic infections of internal organs. An all-too-common trigger for oral or vaginal yeast infections is the use of an antibiotic to treat a bacterial infection. The antibiotic diminishes the nor-mal bacterial flora, thereby removing competition for the yeasts, which are then able to overgrow. Yeasts may also cause skin infections in diabetics, or in obese peo-ple who have skin folds that are always moist. In recent years, Candida has become an important cause of noso-comial infections. The resistance of hospital patients is often lowered because of their diseases or treatments, and they are more susceptible to systemic yeast infec-tions in the form of pneumonia or endocarditis.
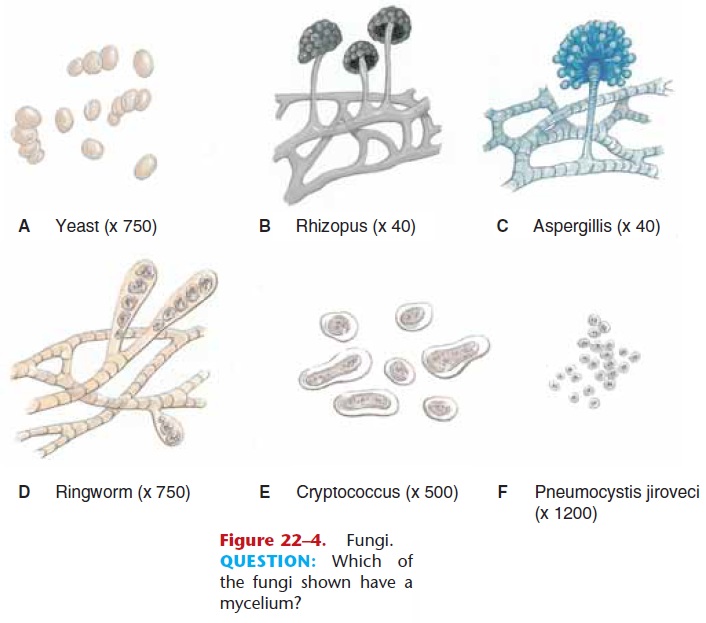
Another superficial mycosis is ringworm (tinea), which may be caused by several species of fungi (see Table 22–5). The nameringworm is misleading, because there are no worms involved. It is believed to have come from the appear-ance of the lesions: circular, scaly patches with red dened edges; the center clears as the lesion grows. Athlete’s foot, which is probably a bacterial-fungal infection, is perhaps the most common form of ring-worm.
The systemic mycoses are more serious diseases that occur when spores of some fungi gain access to the interior of the body. Most of these fungi grow in a mold-like pattern. The molds we sometimes see on stale bread or overripe fruit look fluffy or fuzzy. The fluff is called a mycelium and is made of many thread-like cellular structures called hyphae. The color of a mold is due to the spore cases (sporangia) in which the reproductive spores are produced (see Fig. 22–4). Each spore may be carried by the air to another site, where it germinates and forms another mycelium.
Because spores of these fungi are common in the environment, they are often inhaled. The immune responses are usually able to prevent infection and healthy people are usually not susceptible to systemic mycoses. Elderly people and those with chronic pul-monary diseases are much more susceptible, however, and they may develop lung infections.
The importance of the immune system is clearly evident if we consider people with AIDS. Without the normal immune responses, AIDS patients are very susceptible to invasive fungal diseases, including meningitis caused by Cryptococcus. Pneumocystis jiroveci(formerly P. carinii and classified with the protozoa, its DNA sequences suggest it is closer to the fungi) is an impor-tant cause of pneumonia in people with AIDS. This species is usually not pathogenic, because the healthy immune system can easily control it. For AIDS patients, however, this form of pneumonia is often the cause of death.
Antifungal Medications
One of the most effective drugs used to treat serious, systemic mycoses, amphotericin B, has great potential to cause serious side effects. Patients receiving this medication should have periodic tests of liver and kid-ney function. Newer medications include ketocona-zole, fluconazole, and caspofungin, which are less toxic to the recipient and may prove to be as effective as amphotericin B.
Superficial mycoses such as ringworm may be treated with certain oral medications. Taken orally, the drug is incorporated into living epidermal cells. When these cells die and reach the stratum corneum, they are resistant to the digestive action of the ringworm fungi. An effective topical spray has also been developed.
There are several effective medications for mucosal yeast infections, but it is important that the trigger for the infection (such as antibiotic therapy) be resolved as well. If it is not, the yeast infection may recur when the medication is stopped.
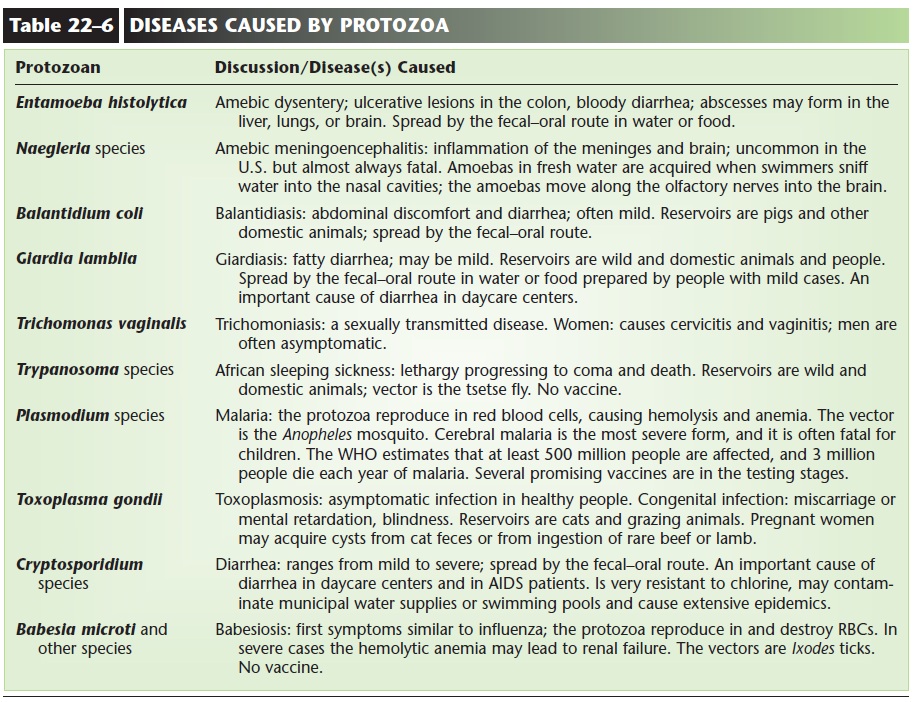
PROTOZOA (SEE TABLE 22–6)
Protozoa are unicellular animals, single cells that are adapted to life in freshwater (including soil) and salt-water. Some are human pathogens and are able to form cysts, which are resistant, dormant cells that are able to survive passage from host to host.
Intestinal protozoan parasites of people include Entamoeba histolytica, which causes amebic dysentery, and Giardia lamblia, which causes diarrhea called giar-diasis (Fig. 22–5 and Table 22–6). People acquire these by ingesting food or water contaminated with the cysts of these species. Giardiasis can become a prob-lem in daycare centers if the staff is not careful con-cerning hand washing and food preparation.
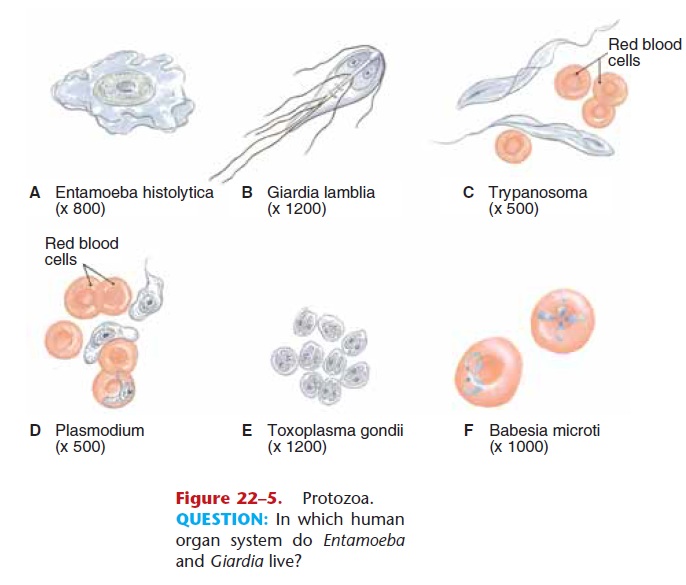
Figure 22–5. Protozoa.
QUESTION: In which human organ system do Entamoeba and Giardia live?
Plasmodium, the genus that causes malaria, affects hundreds of millions of people throughout the world (causing 2 to 3 millions deaths each year) and is prob-ably the most important protozoan parasite. The Plasmodium species are becoming increasingly resist-ant to the standard antimalarial drugs, which are used to prevent disease as well as cure it. Work is progress-ing on several malaria vaccines, and some have shown promise.
Medications are available that can treat most proto-zoan infections. Intestinal protozoa, for example, may be treated with metronidazole or furazolidone.
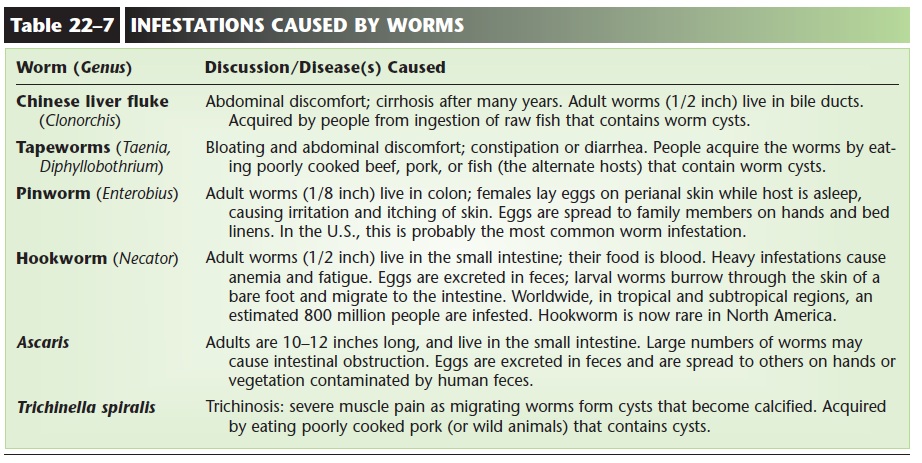
WORMS (HELMINTHS) (SEE TABLE 22–7)
Most worms are simple multicellular animals. The parasitic worms are even simpler than the familiar earthworm, because they live within hosts and use the host’s blood or nutrients as food. Many of the parasitic worms have complex life cycles that involve two or more different host species.
The flukes are flatworms that are rare in most of North America but very common in parts of Africa and Asia. People acquire these species by eating aquatic plants or raw fish in which the larval worms have encysted. Within the person, each species lives in a specific site: the intestine, bile ducts, or even certain veins. Although rarely fatal, these chronic worm infes-tations are often debilitating, and the host person is a source of the eggs of the fluke, which may then infect others.
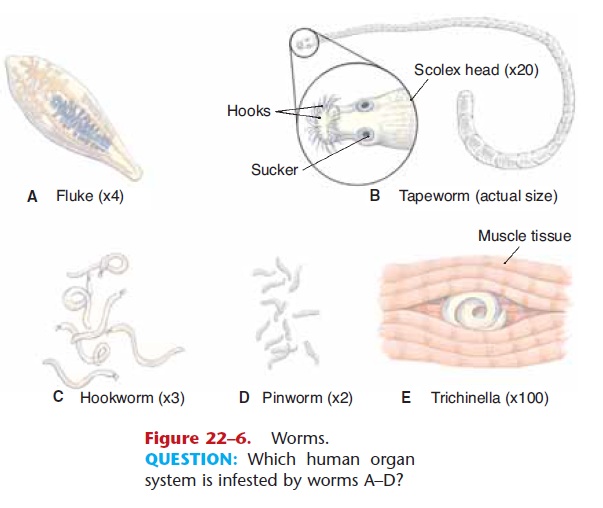
Tapeworms are also flatworms (Fig. 22–6). Some are 10 to 15 feet long, and the fish tapeworm can be as long as 60 feet. They are as flat as a ribbon, however, and one could easily be held in the palm of the hand. The tapeworm holds on to the lining of a host’s small intestine with the suckers and hooks on its scolex (front end). The segments, called proglottids, are produced continuously in most species and absorb nutrients from the host’s digested food. The only function of the proglottids is reproduction: Eggs in one segment are fertilized by sperm from another segment. Mature proglottids containing fertilized eggs break off and are excreted in the host’s feces. An intermediate host such as a cow or pig eats food con-taminated with human feces, and the eggs hatch within this animal and grow into larval worms that encyst in the animal’s muscle tissue. People become infected by eating poorly cooked beef or pork that contains cysts.
Parasitic roundworms of people include hook-worm, pinworm, Ascaris, and Trichinella (see Table 22–7). Medications are avail-able that can eliminate worm infestations. In endemic areas, however, reinfestation is quite common.
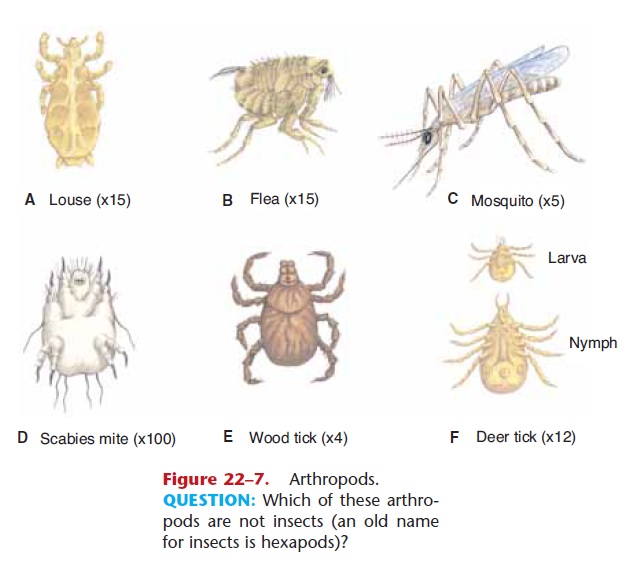
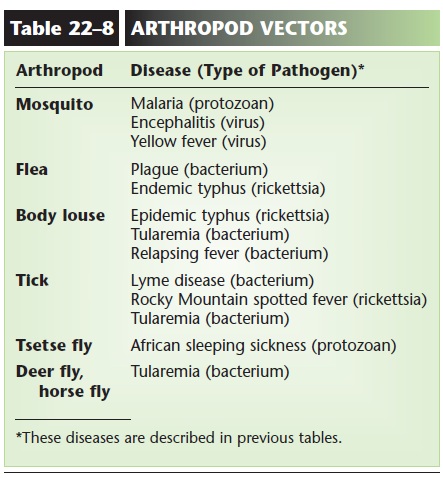
ARTHROPODS (SEE TABLE 22–8)
Arthropods such as the scabies mite and head lice are ectoparasites that live on the surface of the body. The infestations they cause are very itchy and uncom-fortable but not debilitating or life threatening (Fig. 22–7). Of greater importance are the arthropods that are vectors of disease. These are listed in Table 22–8. Mosquitoes, fleas, lice, and flies are all insects. Ticks are not insects but are more closely related to spiders.
Related Topics