Chapter: Modern Medical Toxicology: Asphyxiant Poisons: Toxic Gases
Smoke - Systemic Asphyxiant Poison
Smoke
·
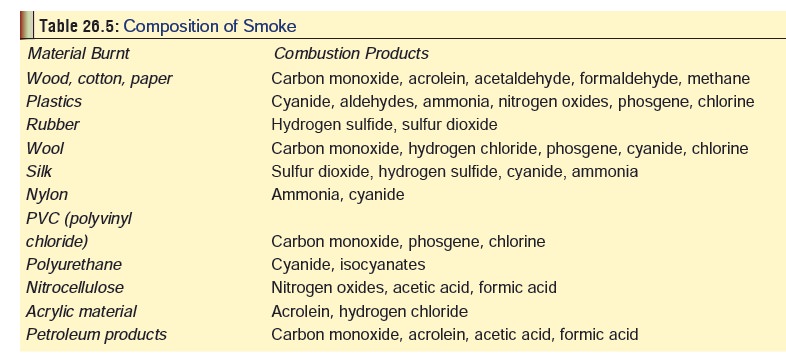
Smoke is defined as a solid aerosol
resulting from the incom-plete combustion (pyrolysis) of any organic matter,
and should be differentiated from “fumes” which refer to a suspension of fine
solid particles in a gas resulting from condensation (e.g. metal oxides
generated during smelting, welding, etc.). The exact composition of smoke
depends on the material burnt (Table
26.5).
Diagnosis
·
Arterial blood gas analysis.
·
Carboxyhaemoglobin and methaemoglobin concentrations.
·
Chest X-ray (may be normal in the early stages). Xenon
ventilation studies can detect small airway and alveolar injury before
radiographic changes become apparent.
·
Spirometry: with special reference to FEV1.
·
Other tests of value include EKG, SMA-6, slit lamp exam of
the eyes, indirect laryngoscopy and pulmonary function tests (Xenon 133 lung
scan, bronchoscopy, and 99mTc DTPA clearance).
Treatment
·
An evaluation of the exposure
setting may help the physician determine the amount and type of toxic
substances to which the victim has been exposed. Factors of potential
importance include open vs closed space, estimated length of exposure, presence
or absence of steam, explosion, nature of burning material and packaging,
status of other victims and the amount, colour, and odour of smoke.
·
Remove victim from environment,
decontaminate, secure airway, ventilate, establish intravenous access, monitor
cardiac rhythm, treat pulmonary oedema and commence burn care if required.
·
Oxygen.
·
Aspirate tracheal secretions.
·
Bronchodilators (parenteral or
nebulised inhalation). Use aminophylline for bronchospasm.
·
Mechanical ventilation, PEEP for
pulmonary oedema.
· Management of CO or cyanide toxicity if present, on conventional lines.
·
Methaemoglobinaemia (more than 20 to
30%) can be treated with methylene blue. The usual adult dose is 1 to 2 mg/kg
IV over 5 minutes, followed by a 15 to 30 ml fluid flush to minimise local
pain. For children, the usual recom-mended dose is 0.3 to 1 mg/kg.
·
Use dexamethasone, mannitol,
furosemide for cerebral oedema.
·
Consider the use of hyperbaric
oxygen, especially in those cases where carbon monoxide and hydrogen cyanide
are thought to be present.
Related Topics