Chapter: Clinical Dermatology: Skin reactions to light
Polymorphic light eruption
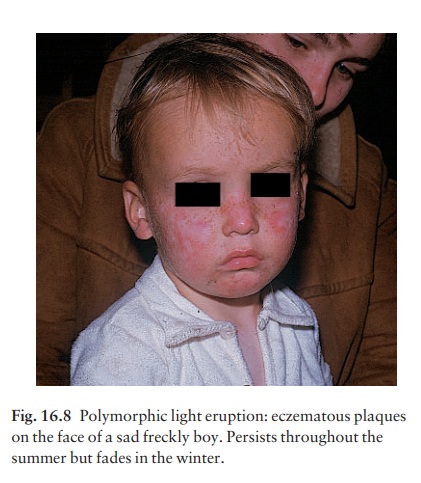
Polymorphic
light eruption
This
is the most frequent cause of a so-called ‘sun allergy’.
Cause
It
is speculated that UVR causes a natural body chem-ical to change into an
allergen. Mechanisms are sim-ilar to those in drug photoallergy.
Presentation
Small
itchy red papulovesicles or eczematous plaques arise from 2 h to 5 days, most
commonly at 24 h, after exposure to UVR. The eruption is itchy and usually
confined to sun-exposed areas (Fig. 16.8), remember-ing that some UVR passes
through thin clothing.
Course
The
disorder tends to recur each spring after UVR exposure. Tanning protects some
patients so that if the initial exposures are limited, few or no symptoms occur
later. Such patients can still enjoy sun exposure and outdoor activities.
Others are so sensitive, or their skin pigments so poorly, that fresh exposures
con-tinue to induce reactions throughout the summer. These patients require
photoprotection, and must limit their sun exposure and outdoor activities. The
rash disappears during the winter.
Differential diagnosis
Phototoxic
reactions, photoallergic reactions, miliaria rubra, chronic actinic dermatitis,
ordinary eczemas, allergic reactions to sunscreens and airborne allergic
contact dermatitis should be considered.
Investigations
It
may be possible to reproduce the dermatitis by test-ing non-sun-exposed skin
with UVB and UVA.
Treatment
If
normal tanning does not confer protection, sunscreens (Formulary 1) should be
used. Protective clothing, such as wide-brimmed hats, long-sleeved shirts and
long trousers, is helpful. In some patients, a 4-week PUVA course in the late spring can create enough tan to
confer protection for the rest of the season. Moderately potent topical
steroids (Formulary 1) usually improve the eruption. Hydroxychloroquine
(Formulary 2) may be effective when used over the sunny season.
Related Topics