Chapter: Psychiatric Mental Health Nursing : Anxiety, Anxiety Disorders, and Stress-Related Illness
Phobias
PHOBIAS
A phobia is an
illogical, intense, and persistent fear of a specific object or a social
situation that causes extreme dis-tress and interferes with normal functioning.
Phobias usu-ally do not result from past negative experiences. In fact, the
person may never have had contact with the object of the phobia. People with
phobias understand that their fear is unusual and irrational and may even joke
about how “silly” it is. Nevertheless, they feel powerless to stop it
(Andreasen & Black, 2006).
People with phobias develop anticipatory anxiety even when thinking
about possibly encountering the dreaded phobic object or situation. They engage
in avoidance behavior that often severely limits their lives. Such avoid-ance
behavior usually does not relieve the anticipatory anxiety for long.
There are three categories of phobias:
·
Agoraphobia (discussed earlier in text)
·
Specific phobia, which is an irrational fear of an object or a
situation
·
Social phobia, which is anxiety provoked by certain so-cial or
performance situations.
Many people express “phobias” about snakes, spiders, rats, or
similar objects. These fears are very specific, easy to avoid, and cause no
anxiety or worry. The diagnosis of a phobic disorder is made only when the phobic
behavior significantly interferes with the person’s life by creating marked
distress or difficulty in interpersonal or occupa-tional functioning.
Specific phobias are subdivided into the following categories:
·
Natural environmental phobias: fear of storms, water, heights, or other natural phenomena
·
Blood-injection phobias: fear of seeing one’s own or
oth-ers’ blood, traumatic injury, or an invasive medical pro-cedure such as an
injection
·
Situational phobias: fear of being in a specific
situation such as on a bridge or in a
tunnel, elevator, small room, hospital, or airplane
·
Animal phobia: fear of animals or insects
(usually a spe-cific type; often this fear develops in childhood and can
continue through adulthood in both men and women; cats and dogs are the most
common phobic objects)
·
Other types of specific
phobias: for example, fear of get-ting lost while driving if not able to
make all right (and no left) turns to get to one’s destination.
In social phobia, also
known as social anxiety disorder, the
person becomes severely anxious to the point of panic or incapacitation when
confronting situations involving people. Examples include making a speech,
attending a social engagement alone, interacting with the opposite sex or with
strangers, and making complaints. The fear is rooted in low self-esteem and
concern about others’ judg-ments. The person fears looking socially inept,
appearing anxious, or doing something embarrassing such as burp-ing or spilling
food. Other social phobias include fear of eating in public, using public
bathrooms, writing in pub-lic, or becoming the center of attention. A person
may have one or several social phobias; the latter is known as generalized
social phobia (Culpepper, 2006).
Onset and Clinical Course
Specific phobias usually occur in childhood or adolescence. In some
cases, merely thinking about or handling a plastic model of the dreaded object
can create fear. Specific phobias that persist into adulthood are lifelong 80%
of the time.
The peak age of onset for social phobia is middle ado-lescence; it
sometimes emerges in a person who was shy as a child. The course of social
phobia is often continuous, although the disorder may become less severe during
adulthood. Severity of impairment fluctuates with life stress and demands.
Treatment
Behavioral therapy works well. Behavioral therapists ini-tially
focus on teaching what anxiety is, helping the client to identify anxiety
responses, teaching relaxation tech-niques, setting goals, discussing methods
to achieve those goals, and helping the client to visualize phobic situations.
Therapies that help the client to develop self-esteem and self-control are
common and include positive reframing and assertiveness training (explained
earlier in text).
One behavioral therapy often used to treat phobias is systematic (serial) desensitization, in which the therapist progressively exposes the client to the threatening object in a
safe setting until the client’s anxiety decreases. During each exposure, the
complexity and intensity of exposure gradually increase, but the client’s
anxiety decreases. The reduced anxiety serves as a positive reinforcement until
the anxiety is ultimately eliminated. For example, for the client who fears
flying, the therapist would encourage the client to hold a small model airplane
while talking about his or her experiences; later, the client would hold a
larger model airplane and talk about flying. Even later exposures might include
walking past an airport, sitting in a parked airplane, and, finally, taking a
short ride in a plane. Each session’s challenge is based on the success
achieved in pre-vious sessions (Andreasen & Black, 2006).
Flooding is a form of rapid
desensitization in which a behavioral
therapist confronts the client with the phobic object (either a picture or the
actual object) until it no longer produces anxiety. Because the client’s worst
fear has been realized and the client did not die, there is little reason to
fear the situation anymore. The goal is to rid the client of the phobia in one
or two sessions. This method is highly anxiety producing and should be
conducted only by a trained psychotherapist under controlled circum-stances and
with the client’s consent.
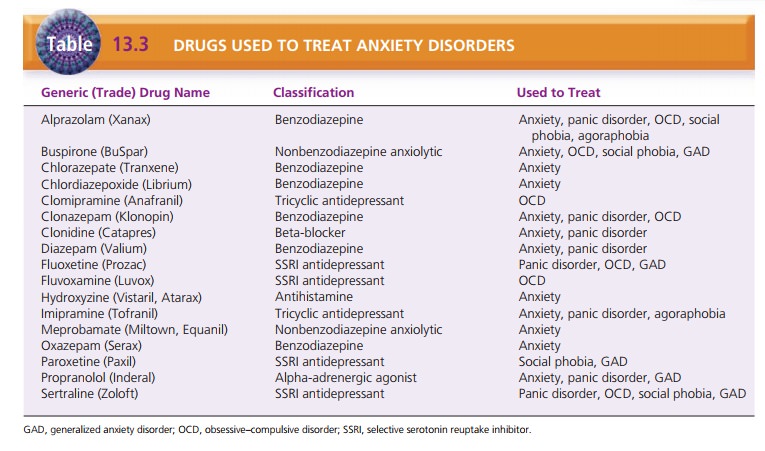
Drugs used to treat phobias are listed in Table 13.3.
Related Topics