Chapter: Psychiatric Mental Health Nursing : Anxiety, Anxiety Disorders, and Stress-Related Illness
Obsessive-Compulsive Disorder
OBSESSIVE–COMPULSIVE DISORDER
Obsessions are recurrent, persistent,
intrusive, and unwanted thoughts,
images, or impulses that cause marked anxiety and interfere with interpersonal,
social, or occupational function. The person knows these thoughts are excessive
or unreasonable but believes he or she has no control over them. Compulsions are ritualis-tic or
repetitive behaviors or mental acts that a person carries out continuously in
an attempt to neutralize anxi-ety. Usually, the theme of the ritual is
associated with that of the obsession, such as repetitive hand-washing when
someone is obsessed with contamination or repeated prayers or confession for
someone obsessed with blas-phemous thoughts. Common compulsions include the
following:
·
Checking rituals (repeatedly making sure the door is locked or the
coffee pot is turned off)
·
Counting rituals (each step taken, ceiling tiles, concrete blocks,
or desks in a classroom)
·
Washing and scrubbing until the skin is raw
·
Praying or chanting
·
Touching, rubbing, or tapping (feeling the texture of each material
in a clothing store; touching people, doors, walls, or oneself)
·
Hoarding items (for fear of throwing away something important)
·
Ordering (arranging and rearranging furniture or items on a desk or
shelf into perfect order; vacuuming the rug pile in one direction)
·
Exhibiting rigid performance (getting dressed in an un-varying
pattern)
·
Having aggressive urges (for instance, to throw one’s child against
a wall).
OCD is diagnosed only when these thoughts, images, and impulses consume
the person or he or she is com-pelled to act out the behaviors to a point at
which they interfere with personal, social, and occupational func-tion.
Examples include a man who can no longer work because he spends most of his day
aligning and realign-ing all items in his apartment or a woman who feels
com-pelled to wash her hands after touching any object or person.
OCD can be manifested through many behaviors, all of which are
repetitive, meaningless, and difficult to con-quer. The person understands that
these rituals are unusual and unreasonable but feels forced to perform them to
alleviate anxiety or to prevent terrible thoughts. Obsessions and compulsions
are a source of distress and shame to the person, who may go to great lengths
to keep them secret.
Onset and Clinical Course
OCD can start in childhood, especially in males. In females, it
more commonly begins in the 20s. Overall, distribution between the sexes is
equal. Onset is usually gradual, although there have been cases of acute onset
with periods of waxing and waning symptoms. Exacer-bation of symptoms may be
related to stress. Eighty per-cent of those treated with behavior therapy and
medica-tion report success in managing obsessions and compulsions, whereas 15%
show progressive deteriora-tion in occupational and social functioning (APA,
2000).
Treatment
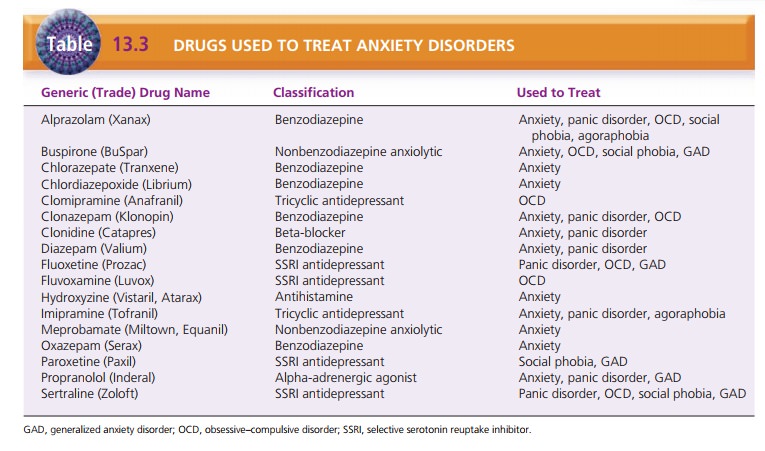
Like for other anxiety disorders, optimal treatment for OCD
combines medication and behavior therapy. Table 13.3 lists drugs used to treat
OCD. Behavior therapy specifically includes exposure and response prevention: Exposure involves assisting the client
to deliberately con-front the situations and stimuli that he or she usually
avoids. Response prevention focuses
on delaying or avoid-ing performance of rituals. The person learns to tolerate
the anxiety and to recognize that it will recede without the disastrous
imagined consequences. Other techniques dis-cussed previously, such as deep
breathing and relaxation, also can assist the person to tolerate and eventually
man-age the anxiety (Bandelow, 2008).
Related Topics