Chapter: Modern Pharmacology with Clinical Applications: Local Anesthetics
Pharmacology of Antispasticity Agents
PHARMACOLOGY OF
ANTISPASTICITY AGENTS
Muscle relaxants have some
value for relief of spastic muscle disorders, that is, a state of increased
muscle tone that results from an imbalance between central and spinal control
of muscle tone. Spasticity is the
result of a general release from supraspinal control and is charac-terized by
heightened excitability of α- and γ-motor sys-tems and the appearance of primitive spinal cord
re-flexes. Treatment is difficult, since relief often can be achieved only at
the price of increased muscle weakness.
Baclofen
Baclofen (Lioresal) is the parachlorophenol
analogue of the naturally occurring neurotransmitter γ-aminobu-tyric acid (GABA).
Mechanism of Action
Baclofen appears to affect
the neuromuscular axis by acting directly on sensory afferents, γ-motor neurons, and
collateral neurons in the spinal cord to inhibit both monosynaptic and
polysynaptic reflexes. The principal effect is to reduce the release of
excitatory neurotrans-mitters by activation of presynaptic GABAB
receptors. This seems to involve a G protein and second-messen-ger link that
either increases K+ conductance or de-creases Ca++ conductance.
Absorption, Metabolism, and Excretion
Baclofen is rapidly and
effectively absorbed after oral administration. It is lipophilic and able to
penetrate the blood-brain barrier. Approximately 35% of the drug is excreted
unchanged in the urine and feces.
Clinical Uses
Baclofen is an agent of choice for treating spinal spastic-ity and
spasticity associated with multiple sclerosis. It is not useful for treating spasticity of supraspinal origin. Doses
should be increased gradually to a maximum of 100 to 150 mg per day, divided
into four doses.
Adverse Effects
Side effects are not a major
problem, and they can be minimized by graduated dosage increases. They include
lassitude, slight nausea, and mental disturbances (in- cluding confusion,
euphoria, and depression). The drowsiness is less pronounced than that produced
by diazepam—an important therapeutic advantage. Hypo-tension has been noted,
particularly following overdose. Elderly patients and patients with multiple
sclerosis may require lower doses and may display increased sen-sitivity to the
central side effects. Baclofen may increase the frequency of seizures in
epileptics.
Benzodiazepines
Benzodiazepines also possess
muscle relaxant activity. Diazepam (Valium)
has been used for control of flexor and extensor spasms, spinal spasticity, and
multiple scle-rosis. The muscle relaxant effect of the benzodiazepines may be
mediated by an action on the primary afferents in the spinal cord, resulting in
an increased level of presynaptic inhibition of muscle tone. Polysynaptic
re-flexes are inhibited. The most troublesome side effect is drowsiness, which
is dose dependent. Tolerance to both the therapeutic effects and the side
effects develops.
Dantrolene Sodium
Dantrolene sodium (Dantrium) is used in the treatment of
spasticity due to stroke, spinal injury, multiple sclero-sis, or cerebral
palsy. It is also the drug of choice in
pro-phylaxis or treatment of malignant hyperthermia. Susceptibility to
malignant hyperthermia is due to a rare genetic defect that allows Ca++
release from the sarcoplasmic reticulum to open more easily and close less
readily than normal. This leads to a high level of Ca++ in the
sarcoplasm, which produces muscle rigidity, oxygen consumption, and heat.
Dantrolene acts by blocking Ca++ release from the sarcoplasmic
reticulum and uncoupling excitation from contraction.
Dantrolene is active orally,
although its absorption is slow and incomplete. Its biological half-life (t1/2)
is 8.7 hours in adults. The drug is metabolized by liver micro-somal enzymes
and is eliminated in the urine and bile. It is given IV when treating an attack
of malignant hy-perthermia.
The most prominent and often
limiting feature of dantrolene administration is dose-dependent muscle
weakness. Other side effects are drowsiness, dizziness, malaise, fatigue, and
diarrhea. Symptomatic hepatitis is reported in 0.5% of patients receiving it
and fatal hepa-titis in up to 0.2%. Contraindications include respira-tory
muscle weakness and liver disease. It is suggested that patients on dantrolene
therapy be given regular liver function tests.
Central Skeletal Muscle Relaxants
The central skeletal muscle
relaxants are a chemically diverse group of compounds that have limited utility
in relieving the signs and symptoms of local muscle spasm. None has been shown
to be superior to analgesic– antiinflammatory agents for the relief of acute or
chronic muscle spasm, although all are superior to placebo. Most of these drugs
have mild sedative prop-erties, and their muscle relaxant activity may be a
direct result of sedation. Experimentally, all
centrally active skeletal muscle
relaxants preferentially depress spinal polysynaptic reflexes over monosynaptic
reflexes.
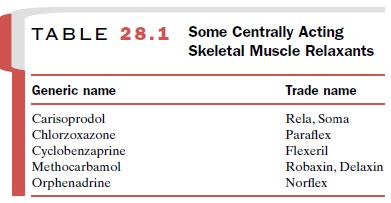
Most of the agents have
similar actions, and there-fore, the same adverse reactions are seen. These
consist most commonly of drowsiness, dizziness, and light-head-edness. One
agent, cyclobenzaprine (Flexeril),
has a prominent anticholinergic component and frequently causes dryness of the
mouth along with sedation and dizziness.In addition to being employed alone,
many of these compounds are available in combination with a nonopi-oid
analgesic, caffeine, or both. Because of their limited utility, they are not be
considered individually. Some of the approved agents are listed in Table 28.1.
Related Topics