Chapter: Paediatrics: Respiratory medicine
Paediatrics: Laryngeal and tracheal inflammation
Laryngeal and tracheal inflammation
There are a number of laryngeal
and tracheal causes of inflammation and airway obstruction. In the acute
setting you will be concerned with three common conditions.
·
Viral laryngotracheobronchitis
(croup): mucosal
inflammation affecting anywhere from
the nose to the lower airway that is commonly due to parainfluenza, influenza,
and respiratory syncytial virus in children aged 6mths to 6yrs.
·
Spasmodic or recurrent croup: barking cough and hyperreactive
upper airways with no apparent
respiratory tract symptoms.
·
Acute epiglottitis: life-threatening swelling of the
epiglottis and septicaemia due to Haemophilus influenzae type b
infection—most commonly in children aged 1–6yrs. This is now rare since routine
HiB immunization.
Diagnosis
History
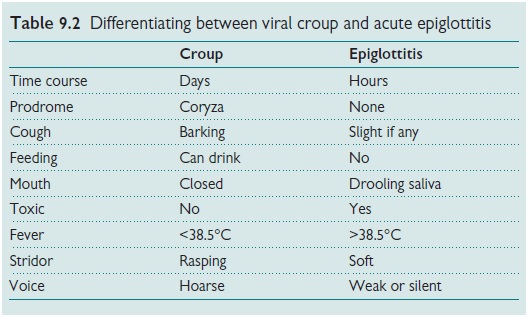
In practice the two main
conditions that require differentiating are
viral croup and acute epiglottitis. The history may help in this process (see
Table 9.2).
Examination
Do
not examine the throat. Take
a careful assessment of severity including:
·
Degree
of stridor and subcostal recession.
·
Respiratory
rate.
·
HR.
·
LOC
(drowsiness), tiredness, and exhaustion.
Pulse oximetry.
Treatment
Priority
The main priority in the emergency
setting is to differentiate between acute epiglottitis and viral croup (see
Table 9.2). If you are unsure, stabilize the child and ensure that nothing
precipitates distress and possible airway obstruction. Try and keep the child,
family, and staff calm. Alert emergency otolaryngologist and anaesthetist to
the possibility of a need for emergen-cy airway support.
Viral croup
Children with mild illness can be
managed at home, but advise parents that if there is recession and stridor at
rest then they will need to return to hospital. Infants <12mths may need
closer attention. Treatments include the following.
·Moist
or humidified air: although
widely used to ease breathing the benefit
of these physical measures is unproven.
·Steroids:
oral prednisolone (2mg/kg for 3
days) or oral dexamethasone (0.15mg/kg
stat dose) or nebulized budesonide (2mg stat dose) reduces the severity and duration
of croup. They are also likely to reduce the need for endotracheal intubation.
·Nebulized
adrenaline (epinephrine): can
provide transient relief of symptoms.
In cases that require endotracheal
intubation steroids should be given and, if there is evidence of secondary
bacterial infection or bacterial tracheitis, antibiotics should be added.
Acute epiglottitis
The child with acute epiglottitis
will need to be managed in the intensive care unit after endotracheal
intubation. Once this procedure has been completed take blood cultures and
start IV antibiotics.
·2nd
or 3rd generation cephalosporin (e.g. cefuroxime, ceftriaxome, or cefotaxime) IV for 7–10 days.
·Rifampicin
prophylaxis to
close contacts.
Related Topics