Chapter: Microbiology and Immunology: Bacteriology: Corynebacterium
Other Pathogenic Corynebacterium Species
Other Pathogenic Corynebacterium Species
Corynebacterium ulcerans
C. ulcerans usually causes skin infections but occasionally isassociated with diphtheria-like lesions, such as pharyngitis and respiratory disease. It resembles C. diphtheriae gravis type, but differs from it by (a) reducing nitrate to nitrite, ( b) liquefying gel-atin, and (c) fermenting trehalose. C. ulcerans produces two types of toxins: one resembles that of C. diphtheriae and other resem-bling that of C. pseudotuberculosis. C. ulcerans is also pathogenic for animals. The bacteria can cause infection in cows, and it can be transmitted to humans through milk. Antidiphtheria toxin con-fers protection against the infection caused by C. ulcerans.
Corynebacterium jeikeium (Group JK)
C. jeikeium can colonize the skin of healthy people. Patients withprolonged hospitalization, neutropenia, or on a prolonged course of antibiotics are more susceptible to colonization by the bacteria. C. jeikeium is an opportunistic pathogen in immunocompromisedpatients with hematological disorders or intravascular catheters. The bacteria enter through the catheters and cause infections in the immunocompromised patients. In these patients, it causes septicemia, foreign body (catheter, prosthesis) infections, and endocarditis. The bacterium is very resistant to commonly used antibiotics.
Corynebacterium urealyticum (Group D2)
C. urealyticum is an important agent of the urinary tractinfection.
· Group D2 has been reported to cause chronic or recurrent cystitis, bladder stones, and pyelonephritis.
· People with prior urinary tract abnormalities or recent urologic procedures are at highest risk for this disease.
These bacteria produce large quantities of the enzyme urease, which splits urea, producing ammonia, thereby making the urine alkaline. This leads to the formation of struvite calculi or stones. These bacteria are increasingly found in patients with immunosuppression, underlying genitourinary disorders, and in those receiving antibiotic therapy.
Corynebacterium riegelii, Corynebacterium amycolatum, and Corynebacterium glucuronolyticum are examples of other urease-producing Corynebacterium species associated with urinary tract infections.
Corynebacterium pseudotuberculosis
C. pseudotuberculosis is closely related to C. diphtheriae and is also pathogenic for animals especially livestock. C. pseudotuberculosis is reported to be normal inhabitant of the anterior nares and skin. The bacteria colonize more on the skin of the immuno-compromised patients than the healthy persons. In immu-nocompromised hosts, C. pseudotuberculosis is associated with both native and prosthetic valve endocarditis, pneumonia, lung abscesses, tracheobronchitis, and suppurative lymph-adenitis. Antimicrobial resistance to antibiotics is also more common in isolates from immunosuppressed patients.
Corynebacterium haemolyticum
C. haemolyticum causes as many as 10% of all pharyngitis casesin patients between 10 and 30 years. The bacteria produce an extracellular toxin that causes an erythrogenic rash associated with the pharyngitis.
Corynebacterium striatum
C. striatum is found on catheters in patients with neutropeniaand malignancies. The bacterium causes respiratory tract infec-tions and foreign body infections. A case of meningitis caused by C. striatum has also been reported recently.
Diphtheroids
Other Corynebacterium species resembling C. diphtheriae may sometimes be mistaken for diphtheria bacilli and are called diphtheroids or nondiphtherial corynebacteria. Diphtheroids are found as commensals in the skin, throat, conjunctiva, and other areas. They are present widely in
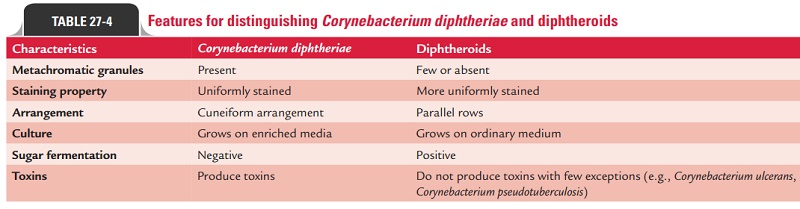
Only recently, the role of these organisms in causing human infec-tions has been recognized. The most common diphtheroids include Corynebacterium xerosisfound in human conjuctival sac, Corynebacterium pseudodiphtheriticum found in human throat; also, these are found to be associated with human infections. Differences between C. diphtheriae and diphthe-roids are summarized in Table 27-4.
Related Topics