Chapter: 12th Nursing : Chapter 7 : Midwifery Nursing
Normal Labour
Normal Labour
Definition
Labour is the process resulting from uterine contraction leading
to expulsion of products of conception from the uterine cavity through vagina.
Normal labour
Labour is called normal when it satisfies the following criteria
·
Spontaneous onset of
labour
·
Starts at 38 – 40 weeks
·
Vertex presentation
·
Occipito-anterior
position
·
Labour is not unduly
prolonged (average 12 hours)
·
No complication to the
mother and baby
Causes of onset of labour
·
The exact mechanisms are
not known. The theories are,
·
Biological – ageing of
conceptus, cell degeneration, hypoxia.
·
Mechanical – myometrial
stretch, decidual cell stretch.
·
Hormonal – prostaglandin
release, oxytocin stimulation, fetal cortisol production and progesterone
withdrawal.
Characteristics of uterine contraction
·
Effective uterine
contraction lasts for 30 – 90 secs create 20 – 30 mmHg of intrauterine pressure
and occur every 2 – 4 minutes.
·
The pain of contraction
is throughout labour to be caused by one or more of the following
·
Hypoxia of the
contracted myometrium.
·
Compression of nerve
ganglia in the cervix and lower uterus by the tightly interlocking muscle
bundles.
·
Stretching of the cervix
during dilatation.
·
Stretching of the
peritoneum overlying the uterus.
Changes in cervix
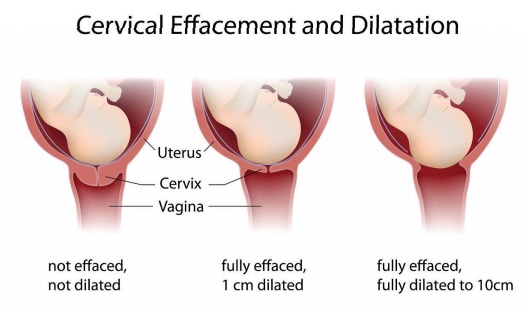
Effacement of the cervix: it is the shortening of the cervix. The
cervix is pulled up and become a part of the uterine segment. Effacement is
expressed as ranging from 0% (no reduction in length) to 100% palpable below
the fetal presenting part.
Dilatation of cervix: cervix dilates to a maximum of 10 cm to
enable the head to pass through the cervix.
Diagnosis Of Labour
True labour pain:
·
Starts over the back
(sacrum) radiates to lower abdomen and thigh.
·
Intermittent colicky
pain.
·
Gradually the intensity,
duration and frequency of contraction increases.
·
Pain is associated with
uterine contraction.
·
Pain is not relieved by
enema.
Dilatation of cervix: Progressive dilatation & effacement
of cervix
Show: Blood stained mucus discharge per vagina due to separation
of the cervical mucus plug.
Stages and Phases Of Labour
First stage: The first stage of labour is the interval
between the onset of true pain and full cervical dilatation. Duration is 6-12
hours. The first stage is further divided into a latent and an active phase.
·
Latent phase:
The latent phase extends from the onset of labour till 3 – 4cm
dilatation. During this phase, uterine contraction are mild and irregular. They
become intense, frequent and regular as the latent phase progress.
·
Active phase:
The active phase is characterized by increased rate of cervical
dilatation.
Second stage: The duration of the 2nd stage averages
2 hours for primi and 30 minutes for multiparaThe 2nd stage of labour is the
interval between full cervical dilatation to delivery of the baby.
Diagnosis of second stage of labour:
·
Bearing down pain with
strong uterine contraction.
·
Bulging of the perineum
and gapping of the anus.
·
Full dilatation of the
cervix.
Third stage: The 3rd stage of labour is the interval
between the delivery of the fetus to delivery of the placenta, umbilical cord
and fetal membranes and lasts 15-30 minutes. Separation of the placenta is the
result of continuous uterine contraction after delivery of the fetus . The
contraction reduces the area of uterine placental bed, with placental
separation occurring in the spongiosa layers of the decidua Vera. Blood loss is
controlled by compression of spiral arteries by the continued contraction which
transport the placenta from fundus into the lower uterine segment and through
cervix into the vagina.
Fourth stage: The 4th stage is the stage of observation
for atleast one hour after the expulsion of the placenta and membranes.
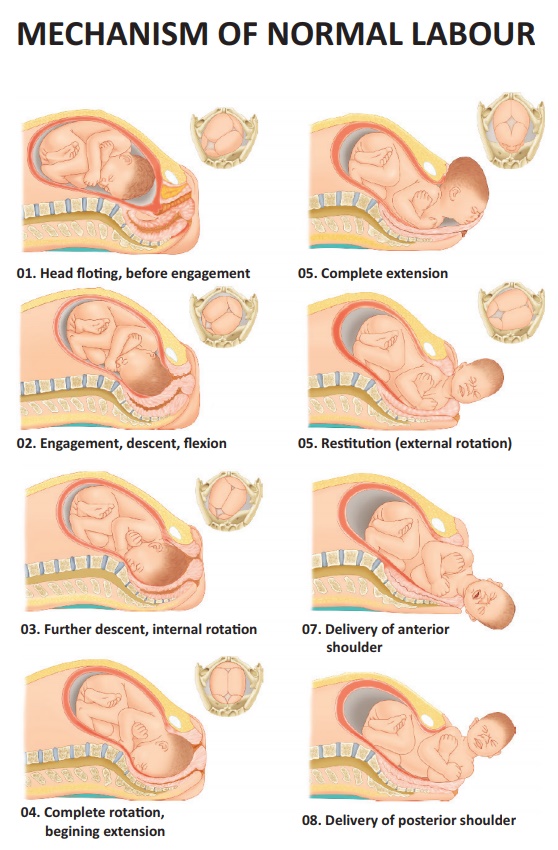
Mechanism Of Normal Labour
Definition: A Series of movements adapted by fetus in the birth
passage during expulsion.
Mechanism of normal labour falls on: - (3 P’s)
·
Power
– strength of
contraction
·
Passage
– pelvic dimensions and
configurations
·
Passenger
– size of the baby
Mechanism
a. Engagement:
When the greatest diameter of the presenting part (biparietal
diameter in vertex) has passed the plane of the pelvic brim, the head is said
to be engaged.It occurs in late pregnancy (primi) or at the time of labour
(multi).
b. Descent:
·
The Presenting part
descends slowly and progressively.It depends on cephalopelvic relationship
c. Flexion:
·
Good flexion aids engagement
and descent.
d. Internal rotation:
·
It occurs on pelvic
floor. The resistance of the pelvic floor helps.
·
The head must rotate to
anterior (or posterior) to pass ischial spines.
e. Crowning:
·
After internal rotation
and further descent, vulva form a crown around the head (i.e.) the biparietal
diameter distends the valval outlet without any recession of the head even
after contraction is over.
f. Extension:
·
Distension of perineum
by vertex.
·
Occiput beyond symphysis
&Head stands out.
g. Restitution:
·
Untwisting of the neck,
head rotates to the position occupied at engagement.
h. External rotation:
·
Shoulder descends in the
path similar to that followed by the head and rotates anteroposteriorly.
·
Head swings.
i. Lateral flexion:
·
Anterior shoulder comes
under the symphysis pubis.
·
Posterior shoulder sweep
the perineum.
j. Expulsion:
After delivery of the shoulder under the symphysis pubis, the rest
of the body expelled quickly. Rest of the body expelled with lateral flexion
Related Topics