Chapter: 12th Nursing : Chapter 7 : Midwifery Nursing
Maternal Physiological Changes During Pregnancy
Maternal Physiological Changes During Pregnancy
Physiological changes during pregnancy.
Genital Organs
Vulva- Vulva becomes oedematous. Labia minoria are pigmented and
enlarged.
Vagina- Vaginal walls becomes oedematous, Because of more blood
supply, the vaginal walls mucosa looks in bluish colour.
Uterus- The uterus which in non-pregnant state, weighs about 60
gm, during pregnancy uterus increases in size upto 10-12kgs.
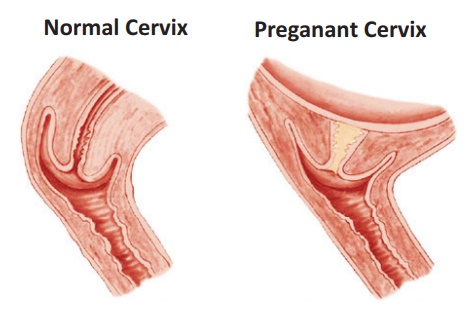
Cervix- Softening of the cervix is evident at 6 weeks. It occurs
due to fluid accumulation inside the fibros tissue of the cervix and increased
vascularity.
Other Organs
Fallopian tube- The total length is increased. The tube
becomes congested.
Ovary- Both the ovarian and uterine cycles of the normal
menstruation remain suspended.
Changes In Breast
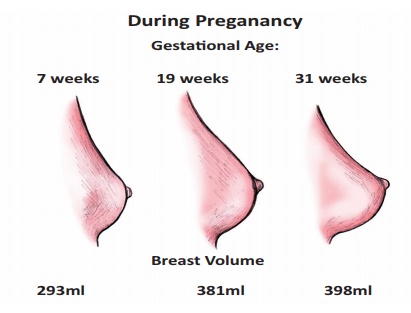
In early pregnancy the women feel fullness of breast or tingle and
increase in size as pregnancy progresses. The areola of the nipples darkens and
the diameter increases. The Montgomery’s glands (the sebaceous glands of the
areola) enlarge and tend to protrude. The surface vessels of the breast may
become visible due to increased circulation. By the 16th week (2nd trimester) the breasts
begins to produce colostrum. It is a thin, watery, yellowish secretion which
thickens as pregnancy progresses. Colostrum may leak from breasts.
Changes In Skin
Skin changes occurs due to increased secretion of Melanocyte
Stimulating Hormone (MSH) from pituitary.
Face- There is an extreme form of pigmentation present around
the cheeck, forehead and around the eyes. It is called as chloasma
gravidarum or pregnancy mask.
Abdomen- A brownish black pigmented line appears on the abdomen
stretching from the Xiphisternum to the symphysis pubis. It will disappear
after delivery (Linea Nigra).
Striae gravidarum-It is a specific form of scarring of the
abdominal skin area due to rapid expansion of the uterus. It looks pinkish in
first pregnancy, in subsequent pregnancy both pinkish and white striae are
visible (Striae albican).
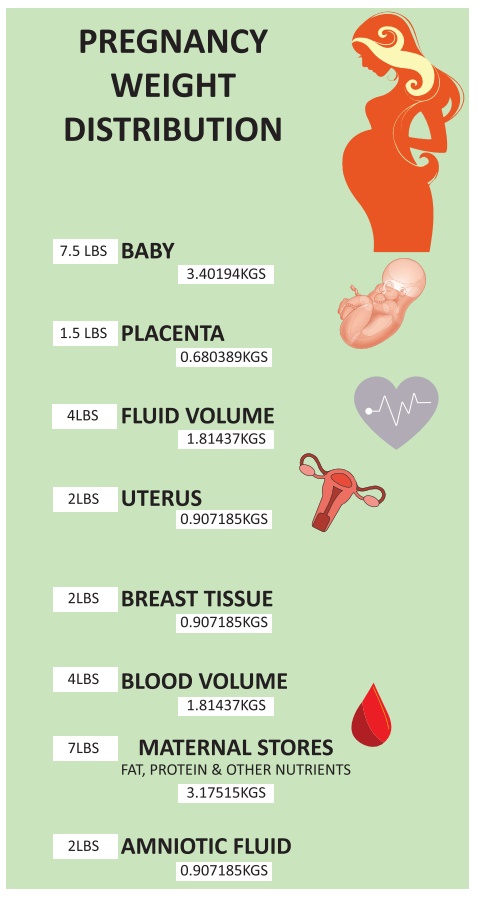
Maternal Weight Gain
The total weight gain during the course of a singleton pregnancy
for a healthy woman averages 11kg. 1kg in first trimester (1-3 months). 5 kg
each in second (4-6 months) and third trimester (7-9 months).
Ideally the weight gain depends on pre-pregnancy body mass index
(BMI) level. Weight gain for a woman with normal BMI (20-26) is 11 to 16kg. An
obese woman (BMI>29) should not gain more than 7 kg. Where as an underweight
woman (BMI<19) may be allowed to gain upto 18kg.
Maternal weight gain 6 kg
·
Increase blood volume
1.3 kg
·
Increase in
extracellular fluid 1.2 kg
·
Accumulation of fat and
protein 3.5 kg
Reproductive weight gain 6 kg
·
Fetus 3.3 kg
·
Placenta – 0.6 kg
·
Liquor (amniotic
fluid)-0.8 kg
·
Uterus-0.9 kg
·
Breast – 0.4 kg
Systemic Changes
Respiratory System:
Because of enlargement of the uterus, there is an elevation of the
diaphragm and breathing becomes diaphragmatic. Upper respiratory tract mucosa
becomes congested. The respiratory rate rises to from 18 to 20 breathes per minute
to meet demand of fetus. Decreased functional residual capacity 1.7 to 1.35
litres due to the compression of the diaphragm by the uterus.
Cardiovascular Changes:
The heart enlarges by 70 to 80ml due to small increase in wall
thickness and venous filling. Cardiac output increases from 4.5 - 6.0
litre/min. Heart rate increases from 70bpm in non-pregnant state to 78bpm at 20
weeks gestation and a peak around 85 bpm in late pregnancy.
Haematological Changes
Blood volume increases by 40-50% at 30-32 weeks of pregnancy. It
causes Haemodilution. Haematocrit decreases. The number of white blood cells
(which fight against infection) increases slightly during pregnancy. Blood
plasma volume increases to the extent of 1.25 litres (Non pregnant plasma
volume is 2500 ml, increase about 3750ml during pregnancy.
Urinary System
·
Glomerular filtration
rate (GFR) is increased by 50% all throughout pregnancy. Frequency of
micturation is a common symptom of early pregnancy. This is due to changes in
pelvic anatomy. A degree of hydronephrosis and hydroureter exist. These result
from the loss of smooth muscle tone due to the progesterone, aggravated by
mechanical pressure from the ureters at the pelvic brim.
·
Vesicoureteric reflux is
also increased. These changes predispose to urinary tract infection.
·
Glycosuria of mild
degree in 35% to 50% of all pregnant woman. Increased glomerular filtration
leads to more sugar reaching the tubules that can be reabsorbed.
Gastrointestinal System
·
The gums become
congested and spongy and may bleed to touch.
·
Relaxation of lower
oesophageal sphincter produces regurgitation and heart burn.
·
Slight reduction in
gastric secretion and diminished gastric motility result in slow emptying and
more effective pulping of food and causes nausea.
·
Reduced motility of
large intestine increased time for water reabsorption which leads to induce
constipation.
Nervous System
·
There may be generalised
neuritis probably due to Vitamin B1 (Thiamine) deficiency.
·
Compression of the
median nerve underneath the carpal ligament over the wrist joint, leading to
pain in the hands and arm called CARPAL TUNNEL SYNDROME may
appear in late pregnancy.
Nausea, vomiting, mental irritability and sleeplessness due to
some psychological background.
Related Topics