Chapter: Obstetrics and Gynecology: Maternal-Fetal Physiology
Maternal Physiology: Respiratory System
Respiratory System
The changes that occur in the
respiratory system during pregnancy are necessitated by the increased oxygen
demand of the mother and fetus. These changes are primarily medi-ated by
progesterone.
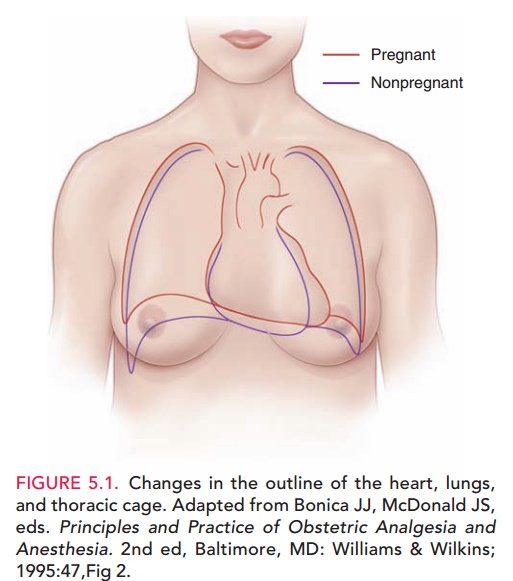
ANATOMIC CHANGES
The
maternal thorax undergoes several morphologic changes due to pregnancy. The
diaphragm is elevated approximately4 cm by late pregnancy due to the enlarging
uterus. Additionally, the subcostal angle widens as the chest diam-eter and
circumference increase slightly (see Figure 5.1).
FUNCTIONAL CHANGES
Pregnancy
is associated with an increase in total body oxygen con-sumption of
approximately 50 mL O2/min, which is 20% greater than nonpregnant
levels. Approximately 50% of this increaseis consumed by
the gravid uterus and its contents, 30% by the heart and kidneys, 18% by the
respiratory muscles, and the remainder by the mammary tissues.
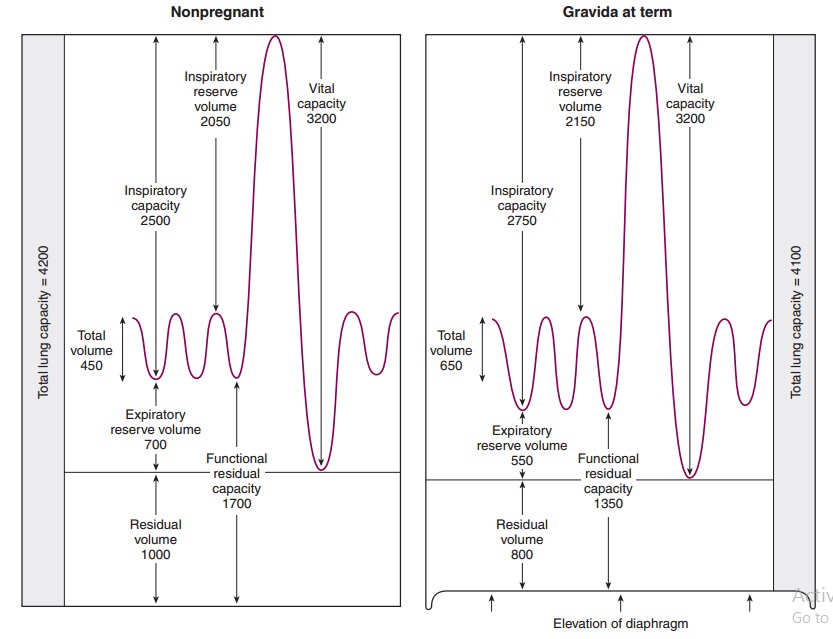
Functional adaptations in the pulmonary system enhance oxygen delivery to the lungs. Figure 5.2 lists res-piratory volumes and capacities associated with pregnancy. The consequence of diaphragmatic elevation is a 20% reduction in the residual volume and functional residual capacity plus a 5% reduction in total lung volume. Although the maternal respiratory rate is essentially unchanged, there is a 30% to 40% increase in tidal volume due to a 5% increase in inspiratory capacity, resulting in a 30% to 40% increase in minute ventilation.

This significant increase in
minute ventilation dur-ing pregnancy is associated with important changes in
the acid–base equilibrium. Progesterone causes increased central chemoreceptor
sensitivity to CO2, which results in increased ventilation and a
reduction in arterial PCO2. The respiratory alkalosis that results
from a decreased arterial PCO2 in pregnancy is compensated by
increased renal excre-tion of bicarbonate, yielding normal pregnancy
bicarbon-ate levels, which means that maternal arterial pH is normal.
SYMPTOMS
Although airway conductance and
total pulmonary resis-tance are reduced in pregnancy, dyspnea is common in pregnant women. Dyspnea of pregnancy is
believed to be a physiologic response to a low arterial PCO2.
Allergy-like symptoms or chronic colds are also common. Mucosal hyperemia
associated with pregnancy results in marked nasal stuffiness and an increased
amount of nasal secretions.
PHYSICAL FINDINGS
Despite the anatomic and
functional changes in the respi-ratory system during pregnancy, no significant
changes in the pulmonary examination are apparent.
DIAGNOSTIC TESTS
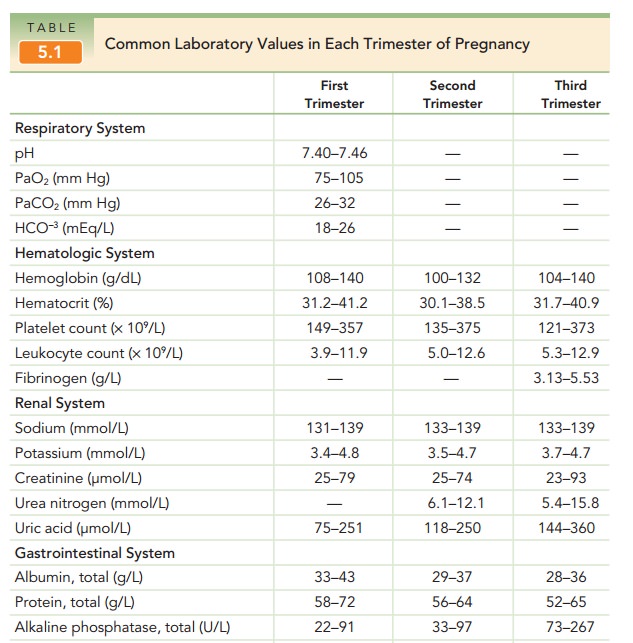
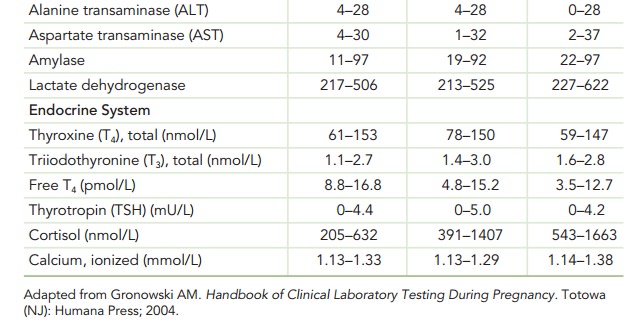
Arterial
blood gas assessment during pregnancy normally shows a compensated respiratory
alkalosis.
Arterial PCO2 levels
of 27 to 32 mm Hg and bicarbonate levels of 18 to 31 mEq/L should be considered
normal.Maternal arterial pH is maintained at normal levels of 7.40 to 7.45 (see
Table 5.1).
During normal pregnancy, chest
radiography may demonstrate prominent pulmonary vasculature due to the
increased circulating blood volume
Related Topics