Chapter: Obstetrics and Gynecology: Isoimmunization
Management of Isoimmunization to Other Red Cell Antigens
MANAGEMENT OF ISOIMMUNIZATION TO OTHER RED CELL ANTIGENS
Although the routine use of Rh
immune globulin has decreased isoimmunization due to the D antigen, iso-immunization due to other blood group
antigens has propor-tionally increased. The frequency of these antibodies
varies depending on the frequency of the antigen in the general population and
in various ethnic groups. In addition, the likelihood that these antibodies
will result in significant fetal hemolytic disease depends on several factors,
includ-ing the size of the sensitizing antigenic stimulus, the rela-tive
potency of the antigen, and the isoform (IgG or IgM) of antibody response.
Sensitization to any of these
antigens can occur in any exposed women lacking the particular antigen,
regardless of her ABO or Rh type. An antibody screen will detect the presence
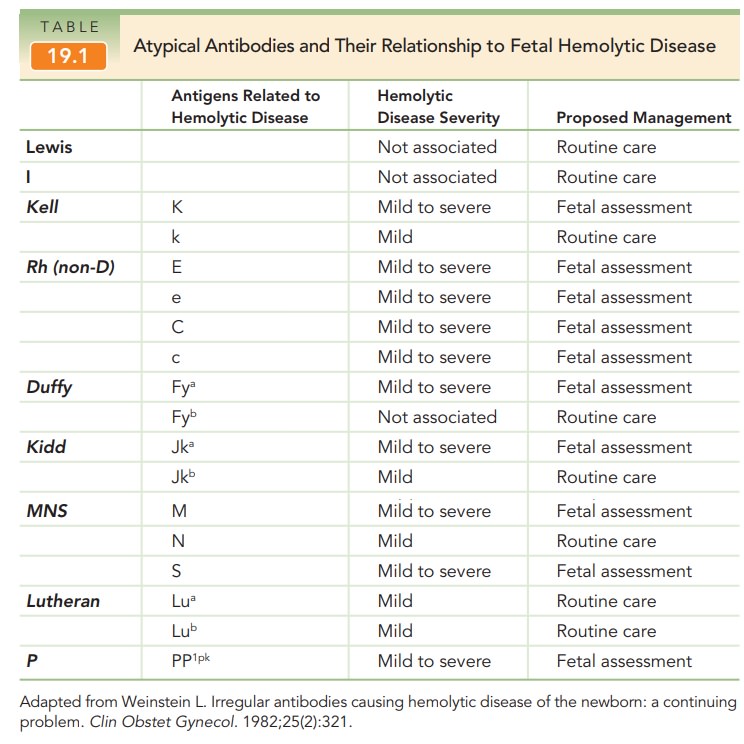
of these antibodies. The most important
cause ofhemolytic disease of the fetus not associated with the D antigen is
isoimmunization to the Kell antigen(see
Table 19.1). Thissensitization commonly results from a prior blood
transfu-sion. If a maternal antibody screen reveals the presence of an
anti-Kell antibody, paternal blood typing for the Kell antigen should be
performed. Because the direct phenotype of the erythrocyte for the Kell antigen
and its complement—the Cellano antigen—can be performed, genotyping is not
necessary. Ninety percent of individuals are Kell-negative, so if paternity is
certain, no further eval-uation is required. Even among those who carry the
Kell antigen, 98% are heterozygous, so consideration should be given to fetal
genotype determination.
Anemia resulting from Kell
isoimmunization is unique in that the predominant effect of the antibody is
destruc-tion and suppression of hematopoietic precursor cells; hemolysis is
only a minimal component of the fetal prob-lem. For this reason, amniotic fluid
surveillance of biliru-bin may not be as useful in monitoring these
pregnancies, and MCA Doppler is the preferred surveillance method. Most
providers use a critical titer measurement of 1:8 to initiate further
evaluation in Kell-sensitized pregnancies.
ABO hemolytic disease, due to maternal-fetal
incompati-bility for the major blood group antigens, can occur. It is
usuallyassociated with mild fetal and newborn hyperbilirubinemia. Typically, it
is not associated with severe fetal disease, because there are fewer A and B
antigenic sites on fetal red blood cells than on adult blood cells. In
addition, much of the anti-A and anti-B antibody produced is of the IgM isoform
that does not cross the placenta to any extent
Related Topics