Chapter: Obstetrics and Gynecology: Fetal Growth Abnormalities:Intrauterine Growth Restriction and Macrosomia
Intrauterine Growth Restriction: Etiology
Etiology
IUGR is a
descriptive term for a condition that has numerous potential causes. Determining
the specific diagnosis is impor-tant for optimal management. Although a number
of causes of IUGR have been recognized, a definite etiology of IUGR cannot be
identified in approximately 50% of all cases. In addition, because the
utilization of a percentile cut-off of 10% alone will result in a high
proportion of false-positives, two-thirds or more of such fetuses categorized
as IUGR will be simply constitutionally small and otherwise healthy.
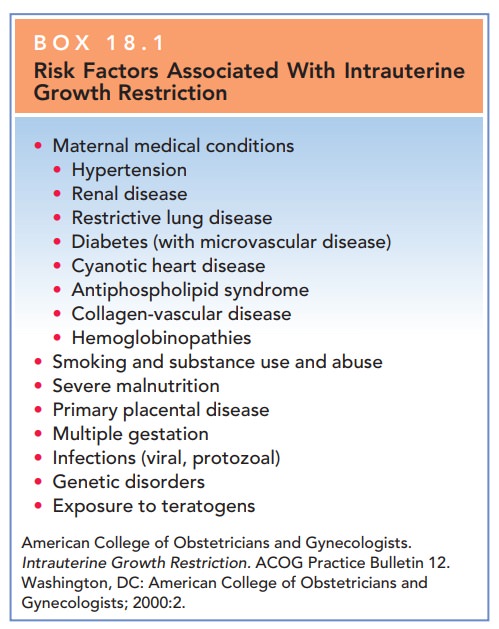
Factors that affect fetal growth
are extensive and include maternal, fetal, and placental causes; these are
listed in Box 18.1.
MATERNAL FACTORS
Maternal factors include viral
infections, such as rubella, varicella, and cytomegalovirus, which are
associated with high rates of growth restriction, particularly if infection
occurs early in pregnancy. Although these infections may manifest only as mild
“flu-like” illnesses, injury to the fetus during organogenesis can result in a
decreased cell number, resulting in diminished growth with or without multiple
congenital anomalies. Five percent or fewer of all cases of IUGR are related to
early infection with these or other viral agents. Maternal substance abuse
affects fetal growth and almost all infants with fetal alcohol syn-drome will
be growth-restricted. Women who smoke during pregnancy deliver babies 200 g
smaller on average than do women who do not smoke; moreover, the rate of growth
restriction is 3- to 4-fold greater among babies born to women who smoke during
pregnancy. Women who use narcotics, heroin, methadone, or cocaine also have
rates of growth-restricted babies ranging from as much as 30% to 50%.
Medications known to be associ-ated with IUGR include anticonvulsant
medications, warfarin, and folic acid antagonists. Altitude may also affect
fetal growth.
Other maternal factors that
affect fetal growth and body composition include demographic factors and
med-ical conditions. Extremes in maternal age (age younger than 16 years and
older than 35 years) are associated with an increased risk of fetal growth
restriction. Medical conditions that alter or affect placental function may
also be causative factors.
Although one common pathway has
not been clearly identified, many of these disorders occur together. Women with
a history of prior obstetric complications have an increased risk of growth
abnormalities. Maternal metabo-lism and body composition are two of the
strongest regula-tors of fetal growth. Nutritional deficiencies and inadequate
weight gain, particularly in teens or in underweight women, may result in IUGR.
FETAL FACTORS
The inherent growth potential of
the individual is deter-mined genetically. Female fetuses are at greater risk
for IUGR than males. In addition, up to 20% of growth-restricted fetuses have a
chromosomal abnormality. In addition, single-gene mutations such as the
glucokinase gene mutation, or genetic syndromes such as Beckwith-Wiedemann
syndrome can also result in abnormalities of growth. Finally, multifetal
pregnancies are at increased risk for growth restriction.
PLACENTAL FACTORS
The placenta is critical for
nutrient regulation and trans-portation from mother to fetus. Abnormalities in
placenta-tion or defective trophoblast invasion and remodeling may contribute
to fetal growth restriction as well as other dis-orders of pregnancy. In
addition, uterine anomalies (uter-ine septum or fibroids) may limit placental
implantation and development and, consequently, nutrient transport, result-ing
in inadequate nutrition for the developing fetus. Finally, the genetic
composition of the placenta is important and abnormalities such as confined
placental mosaicism are asso-ciated with growth delay.
Related Topics