Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Hypertension
Hypertensive Crises
Hypertensive Crises
There
are two hypertensive crises that require nursing interven-tion: hypertensive
emergency and hypertensive urgency. Hyper-tensive emergencies and urgencies may
occur in patients whose hypertension has been poorly controlled or in those who
have abruptly discontinued their medications. Once the hypertensive crisis has
been managed, a complete evaluation is performed to review the patient’s
ongoing treatment plan and strategies to min-imize the occurrence of subsequent
hypertensive crises.
HYPERTENSIVE EMERGENCY
Hypertensive emergency is a situation in which blood pres-sure must
be lowered immediately (not necessarily to less than 140/90 mm Hg) to halt or
prevent damage to the target organs. Conditions associated with hypertensive
emergency include acute myocardial infarction, dissecting aortic aneurysm, and
in-tracranial hemorrhage. Hypertensive emergencies are acute, life-threatening
blood pressure elevations that require prompt treatment in an intensive care
setting because of the serious target organ damage that may occur. The
medications of choice in hyperten-sive emergencies are those that have an
immediate effect. Intra-venous vasodilators, including sodium nitroprusside
(Nipride, Nitropress), nicardipine hydrochloride (Cardene), fenoldopam mesylate
(Corlopam), enalaprilat (Vasotec I.V.), and nitro-glycerin (Nitro-Bid IV,
Tridil), have an immediate action that is short lived (minutes to 4 hours), and
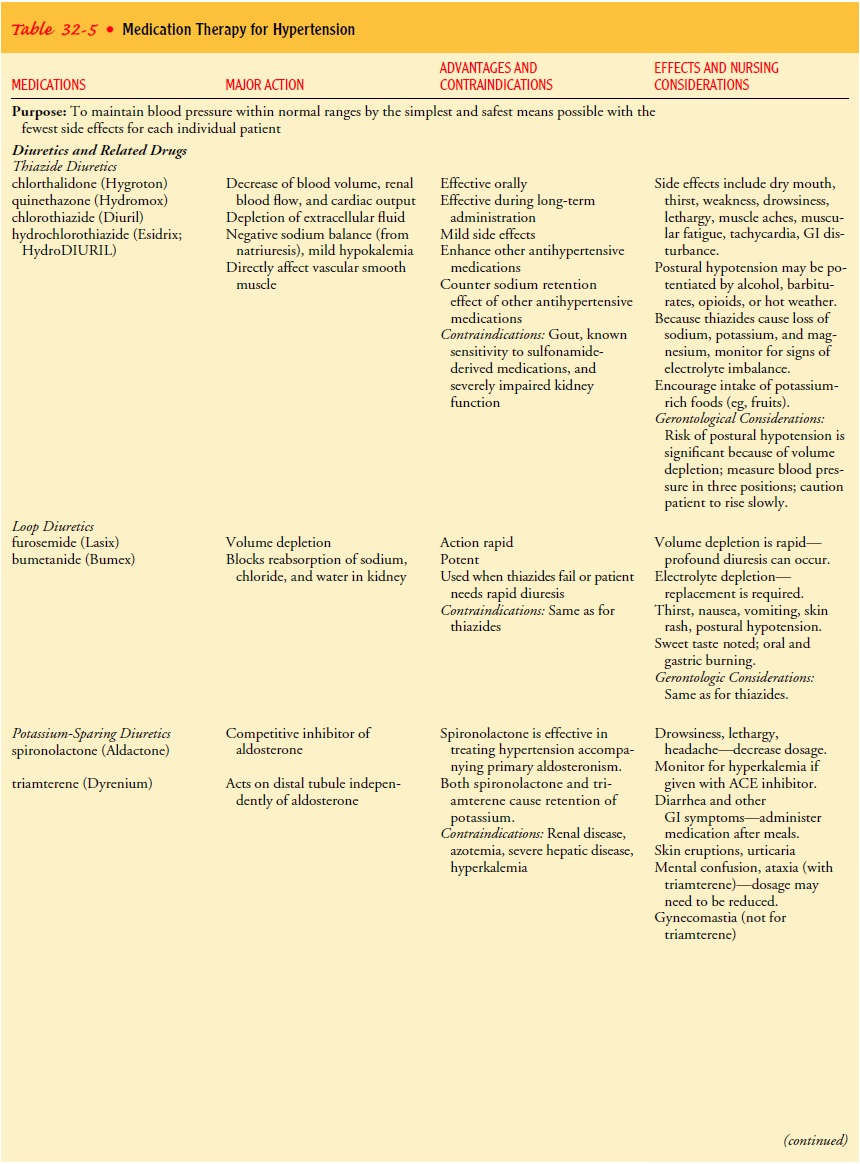
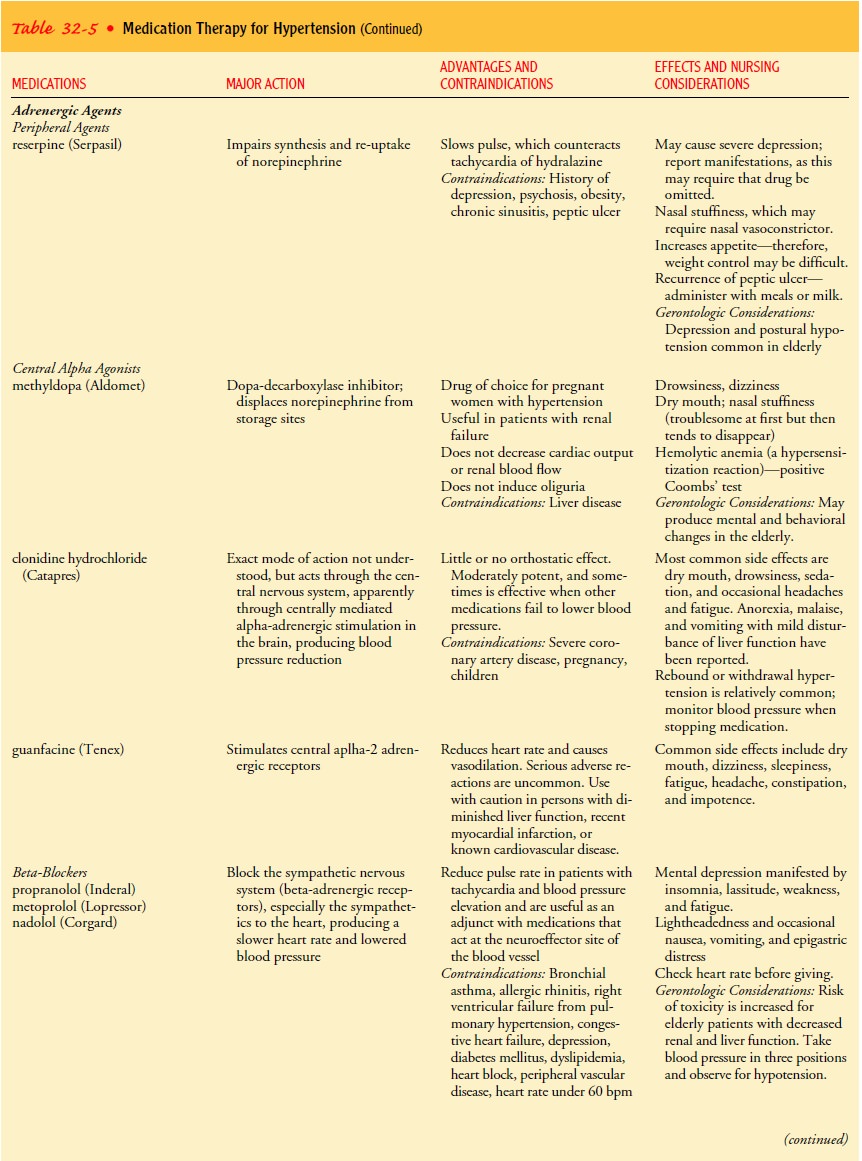
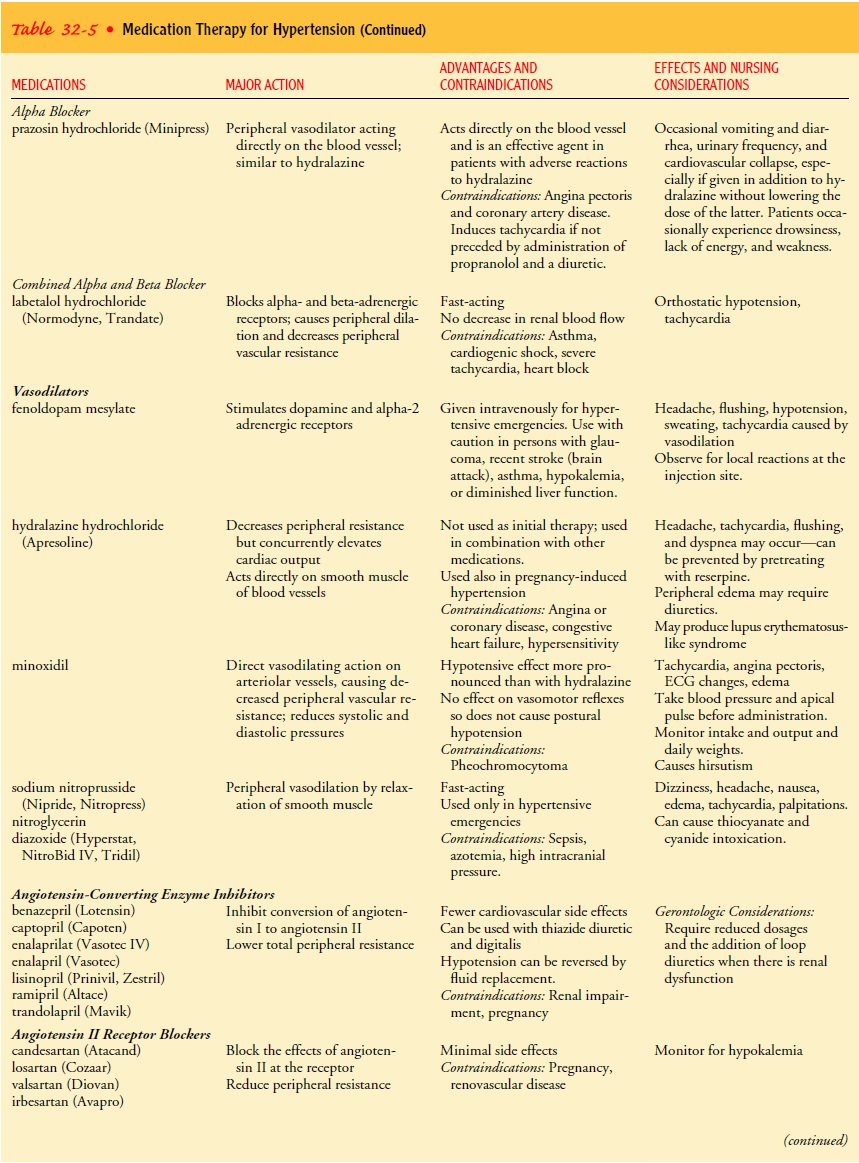
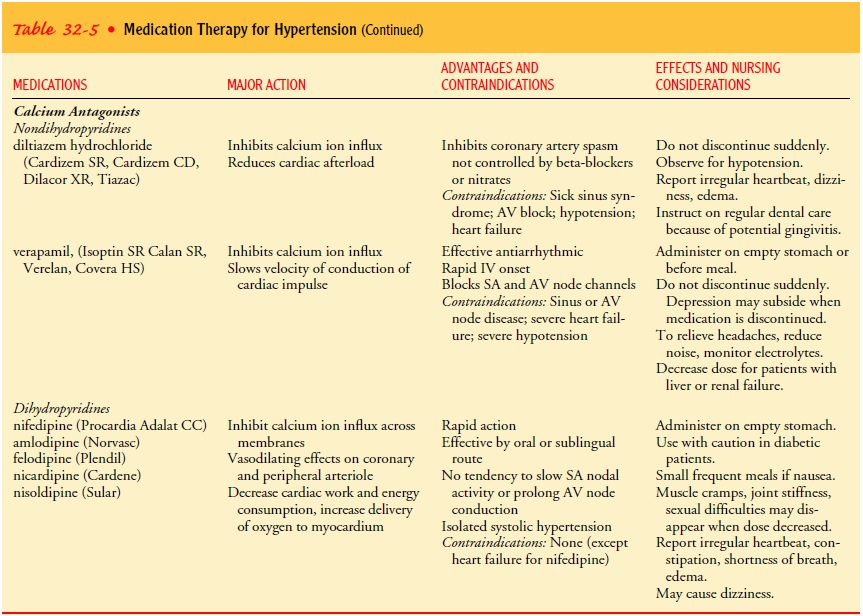
they are therefore used as the initial treatment. Table 32-5 provides for more
information about these medications.
HYPERTENSIVE URGENCY
Hypertensive urgency is a situation in which blood pressure mustbe
lowered within a few hours. Severe perioperative hypertension is considered a
hypertensive urgency. Hypertensive urgencies are managed with oral doses of
fast-acting agents such as loop diuret-ics (bumetanide [Bumex], furosemide
[Lasix]), beta-blockers pro-pranolol (Inderal), metoprolol (Lopressor), nadolol
(Corgard),angiotensin-converting enzyme inhibitors (benazepril [Lotensin],
captopril [Capoten], enalapril [Vasotec]), calcium antagonists (dil-tiazem
[Cardizem], verapamil [Isoptin SR, Calan SR, Covera HS]), or alpha2-agonists, such as
clonidine (Catapres) and guanfacine (Tenex) (see Table 32-5).
Extremely
close hemodynamic monitoring of the patient’s blood pressure and cardiovascular
status is required during treatment of hypertensive emergencies and urgencies.
The exact frequency of monitoring is a matter of clinical judgment and varies
with the patient’s condition. The nurse may think that taking vital signs every
5 minutes is appropriate if the blood pressure is changing rapidly or may check
vital signs at 15 or 30 minutes intervals if the situation is more stable. A
precipitous drop in blood pressure can occur, which would require immediate
action to restore blood pressure to an acceptable level.
Related Topics