Chapter: Basic & Clinical Pharmacology : Introduction to Toxicology: Occupational & Environmental
Herbicides - Specific Chemicals
HERBICIDES
Chlorophenoxy Herbicides
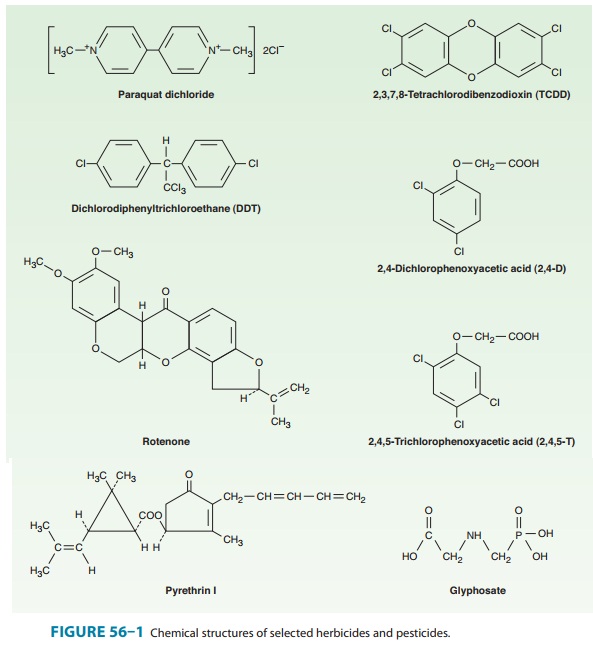
2,4-Dichlorophenoxyacetic acid
(2,4-D), 2,4,5-trichlorophe-noxyacetic acid (2,4,5-T), and
their salts and esters are com-pounds of interest as herbicides used for the
destruction of weeds (Figure 56–1). They have been assigned toxicity ratings of
4 or 3, respectively, which place the probable human lethal dosages at 50–500
or 500–5000 mg/kg, respectively.
Because 2,4,5-T is
often contaminated with dioxins and other polychlorinated compounds, it is no
longer used. It was the com-pound used in “Agent Orange” and caused severe
agricultural damage and social disruption.
In humans, 2,4-D in
large doses can cause coma and general-ized muscle hypotonia. Rarely, muscle
weakness and marked hypotonia may persist for several weeks. In laboratory
animals, signs of liver and kidney dysfunction have also been reported with
chlorphenoxy herbicides. Several epidemiologic studies performed by the US
National Cancer Institute confirmed the causal link between 2,4-D and non-Hodgkin’s
lymphoma. Evidence for a causal link to soft tissue sarcoma, however, is
considered equivocal.The toxicologic profile for these agents, particularly
that of 2,4,5-T, is complicated by the presence of chemical contaminants (dioxins) produced during the manufacturing
process . 2,3,7,8-Tetrachlorodibenzo-p-dioxin
(dioxin, TCDD) is the mostimportant of these contaminants. Dioxin is a potent
animal car-cinogen and a likely human carcinogen.
Glyphosate
Glyphosate
(N-[phosphonomethyl] glycine, Figure
56–1) is now the most widely used herbicide in the world. It functions as a
contact herbicide and is absorbed through the leaves and roots of plants.
Because it is nonselective, it may damage important crops even when used as
directed. Therefore, genetically modified plants such as soy-bean, corn, and
cotton that are glyphosate-resistant have been devel-oped and patented. They
are widely grown throughout the world.Glyphosate-related poisoning incidents are commonly reported.
Most injuries are minor, although some lethal outcomes have been
reported.Glyphosate is a significant eye and skin irritant. It has caused
lethal outcomes, although it is far less potent than the bipyridyl herbicides.
Although the pure chemical seems to have little persis-tence and lower toxicity
than other herbicides, the commercial formulations of glyphosate often contain
surfactants and other active compounds that complicate the toxicity of the
product. No specific treatment is available for glyphosate toxicity.
Bipyridyl Herbicides
Paraquat is
the most important agent of this class (Figure 56–1).Its mechanism of action is
said to be similar in plants and animals and involves single-electron reduction
of the herbicide to free radical species. It has been given a toxicity rating
of 4, which places the probable human lethal dosage at 50–500 mg/kg. Lethal
human intoxications (accidental or suicidal) have been reported. Paraquat
accumulates slowly in the lung by an active process and causes lung edema,
alveolitis, and progressive fibrosis. It probably inhibits superoxide
dismutase, resulting in intracellular free radical oxygen toxicity.In humans, the first
signs and symptoms after oral exposure are hematemesis and bloody stools.
Within a few days, however, delayed toxicity occurs, with respiratory distress
and the develop-ment of congestive hemorrhagic pulmonary edema accompanied by
widespread cellular proliferation. Hepatic, renal, or myocardial involvement
may also be evident. The interval between ingestion and death may be several
weeks. Because of the delayed pulmo-nary toxicity, prompt removal of paraquat
from the digestive tract is important. Gastric lavage, the use of cathartics,
and the use of adsorbents to prevent further absorption have all been
advocated; after absorption, treatment is successful in fewer than 50% of
cases. Oxygen should be used cautiously to combat dyspnea or cyanosis, because
it may aggravate the pulmonary lesions. Patients require prolonged observation,
because the proliferative phase begins 1–2 weeks after ingestion. Management of
severe paraquat poisoning is complex and largely symptomatic. Many approaches
have been used, including immunosuppressive therapy to slow or stop the
progressive pulmonary fibrosis. None of the currently proposed methods of
treatment is universally successful.
Related Topics