Chapter: Essentials of Psychiatry: Individual Psychoanalytic Psychotherapy
Gender and Ethnocultural Issues in Psychotherapy
Gender Issues in Psychotherapy
Does the
gender of the psychotherapist have any effect on the psy-chotherapeutic
relationship and treatment outcome? Are certain psychological problems best
treated by therapists whose gender is different from that of the patient? Do
different phenomena ap-pear in the treatment of those patients whose therapists
are of the same gender? Is the duration of treatment affected by the
thera-pist’s gender? Does gender have any influence on the choice of therapist
by a patient? These are important questions that have been debated in
psychotherapy and psychoanalytic literature for more than 50 years
Although
the literature regarding the advantages and dis-advantages of gender matching
of patients and therapists consists largely of anecdotal and negative reports
(Zlotnick et al., 1998), it is
nevertheless evocative. A number of common themes have emerged, including that
·
The gender of the therapist may be more critical in
supportive treatments that rely on identification with the therapist (Cave-nar
and Werman, 1983).
·
The therapist’s gender may be less important in
psychoa-nalysis than in face-to-face psychoanalytic psychotherapies because, in
the latter, the transference can be less intense (Mogul, 1982).
·
Beginning women therapists have less difficulty
with empathy but more difficulty with authority issues than do their male
counterparts (Kaplan, 1979).
Although
there is only one controlled study and it showed no difference regarding the
influence of the therapist’s gender on the therapeutic process (Zlotnick et al., 1996), there is much to
con-sider about the influence of actual gender and gender-related beliefs of
both patient and therapist on the emergence of transference and
countertransference. However, the best psychoanalytic psychother-apies will
include ample opportunities for the working through of the patient’s issues
related to important figures of both genders
Ethnocultural Issues in Psychotherapy
Culture
refers to meanings, values and behavioral norms that are learned and
transmitted in the dominant society and within its social groups. Culture
powerfully influences cognitions, feel-ing and “self” concept, as well as the
diagnostic process and treatment decisions. Ethnicity, a related concept, refers
to social groupings which distinguish themselves from other groups based on
ideas of shared descent and aspirations, as well as to behav-ioral norms and
forms of personal identity associated with such groups (Mezzich et al., 1993).
Given the
increasing multiculturalism of many cities in the USA, how should the
psychoanalytic psychotherapist treat pa-tients from cultures other than his or
her own? Whereas therapists are obligated to be culturally informed, Foulks and
colleagues (1995) have argued against the promotion of culturally specific
psychotherapies. Although acknowledging that some cross-cul-tural psychiatrists
believe expressive–supportive psychotherapy to be an ethnotherapy appropriate
only to the citizens of the West-ern world, they emphasized the overwhelming
problems in estab-lishing separate therapies and clinics devoted to patients
from a multitude of specific cultures.
Is Psychoanalytic Psychotherapy Effective?
The short
answer to this question is yes. Meta-analytical studies of psychotherapy have
demonstrated unequivocally that psycho-therapy is effective (Luborsky et al., 1975; Smith et al., 1980; Lambert et al.,
1986). The study by Smith and coworkers (1980), for example, demonstrated that
80% of those patients treated in psychotherapy fared better on outcome measures
than those who received no treatment. Psychological growth achieved through
psychotherapy is also enduring (Husby, 1985).
Cost-offset
studies have repeatedly demonstrated the help-fulness of psychotherapy in
reducing general health care services by as much as one-third (Mumford et al., 1984; Krupnick and Pincus, 1992;
Olfson and Pincus, 1994). These include reduction in hospital stays for
surgical and cardiac patients (Mumford et
al., 1982) and decreased treatment costs for those with respiratory
ill-nesses, diabetes and hypertension (Schlesinger et al., 1983). Brief psychotherapy has also been shown to be
effective in general medical clinics, where those patients with significant
medical and psychiatric problems improve substantially more than those treated
by primary care physicians alone (Meyer et
al., 1981).
Luborsky
and coworkers (1993) have demonstrated that psychoanalytic psychotherapy is as
effective as cognitive, behav-ioral, experiential, and group therapies and
hypnotherapy. For this meta-analysis, rigorous inclusion criteria were
established including, but not limited to, adequate sample size with random
assignment, suitable length and frequency of sessions, sound out-come measures,
adherence by therapists to treatment manuals, and comparable skill levels among
therapists. A number of other studies have demonstrated positive benefits in panic
disorder de-pression, personality disorder, drug abuse, eating disorders and
others (Willborg and Dahl, 1996; Bateman and Fonagy, 2001.)
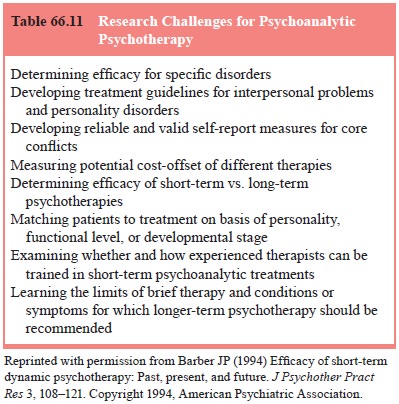
The
important research questions with respect to brief psychoanalytic psychotherapy
have been summarized by Barber (1994) and are relevant to all psychoanalytic
psychotherapies (Table 66.11).
Towards a Neurobiology of Psychotherapy
Exciting new research in psychiatry, brain imaging, cognitive neuroscience, genetics, and molecular biology has provided striking insights into how psychotherapy actually changes both brain structure and function (Liggan and Kay, 1999; Gabbard, 2000; Lehrer and Kay, 2002). Learning and memory are asso-ciated with alterations in central nervous system (CNS) neuro-nal plasticity including increased synaptic strength and number of synapses. Neurogenesis, or the creation of new brain cells, occurs daily in the human hippocampus (Eriksson et al., 1998),
the
central location for the formation of new explicit memories. Not only does memory
consolidation lead to persistent modfica-tions in synaptic plasticity, but
psychotherapy, a form of learn-ing, also produces changes in the permanent
storage of informa-tion acquired throughout an individual’s life and provides
new resources to address important psychobiological relationships between
affect, attachment and memory which is of funda-mental importance in
psychiatric disorders. Rapidly accruing knowledge about the different types of
memory and the role of the amygdala now support the influence of memories that
reside outside of the awareness of our patients (LeDoux, 1996). Implicit
memories formed in infancy and childhood persistently affect the manner in
which patients experience themselves and their worlds as manifested, for
example, in transference reactions within and outside of the therapeutic
relationship.
The study
of psychotherapy from a neurobiological per-spective is likely to provide
greater understanding of how words in the context of therapeutic relationships
can heal. It may be that there are similar mechanisms and anatomical regions
that are involved in the successful treatment of psychiatric illness with
psychotherapy and pharmacotherapy as monotherapies, as well as in the combined
treatment situation (Sacheim, 2001). It is also likely to yield a greater
understanding of pathogenesis and de-lineate helpful interventions to decrease
genetic vulnerability to emotional disorders.
Related Topics