Chapter: Obstetrics and Gynecology: Ovarian and Adnexal Disease
Fallopian Tube Disease
FALLOPIAN TUBE DISEASE
Normal
fallopian tubes cannot be palpated and usually are not con-sidered in the
differential diagnosis of adnexal disease in the asymp-tomatic patient. Common
problems involving the fallopiantubes include ectopic pregnancy,
salpingitis/hydrosalpinx/ tubo-ovarian abscess, and endometriosis (which can
pre-sent as masses or be symptomatic).
Benign Disease of the Fallopian Tube and Mesosalpinx
Paraovarian
cysts develop in the mesosalpinx from vesti-gial Wolffian
duct structures, tubal epithelium, and peri-toneum inclusions. These are
differentiated from paratubal cysts, which are found near the fimbriated end of
the fal-lopian tube, are common, and are called hydatid cystsof Morgagni. Both are usually small and
symptomatic,although, rarely, they can reach large proportions.
Carcinoma of the Fallopian Tube
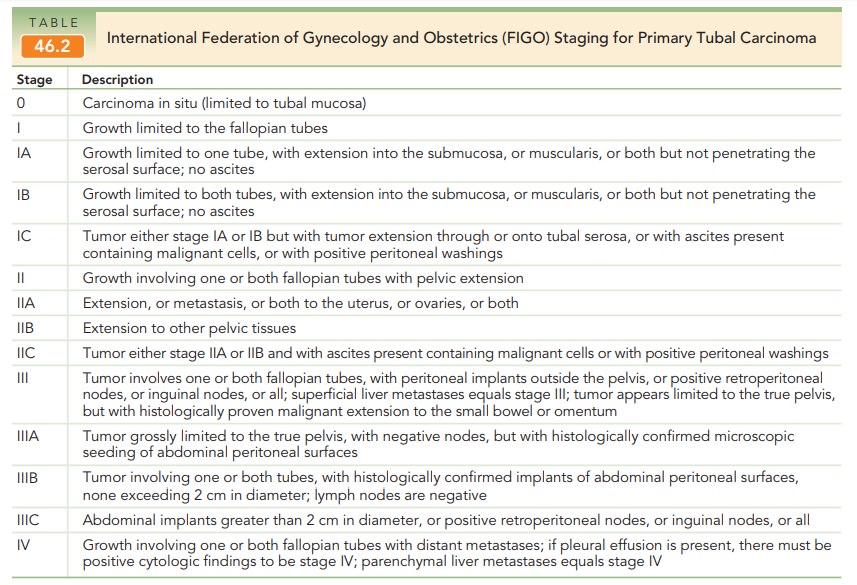
Primary fallopian tube carcinoma is usually an adenocar-cinoma, although other cell types, including adenosqua-mous carcinoma and sarcoma, are rarely reported. About two-thirds of patients with this rare gynecologic cancer (<1% of gynecologic cancers) are postmenopausal. Grossly, these tumors are often rather large, resembling a hydro-salpinx, and unilateral. Microscopically, most are typical papillary serous cystadenocarcinomas of the ovary. The symptoms of this tumor are so slight that the tumor is often advanced before a problem is recognized. The most common complaint associated with fallopian tube carci-noma is postmenopausal bleeding, followed by abnormal vaginal discharge. Profuse serosanguineous discharge, called hydrotubae profluens, is sometimes considered diagnosticof this tumor; however, other findings are watery vaginal discharge, pain, and pelvic mass. Staging is surgical, similar to that for ovarian carcinoma (Table 46.2); progression is similar to that of ovarian carcinoma, with intraperitoneal metastases and ascites. Because the fallopian tubes are richly permeated with lymphatic channels, para-aortic and pelvic lymph node spread often occurs. Seventy percent of fallopian tube cancers present as stage I or II disease. The overall 5-year survival rate is 35% to 45%, with stage I having the most favorable rate. Too few data are available to ascertain whether adjunctive therapy is useful, and this management must be made on a case-by-case basis; how-ever, initial management with staging and debulking is the same as for ovarian cancer treatment.
Carcinoma
metastatic to the fallopian tube, com-ing mainly from the uterus
and ovary, is far more com-mon than primary fallopian tube carcinoma. Other
rare tumors of the fallopian tube include malignant mixed müllerian tumors,
primary choriocarcinoma, fibroma, and adenomatoid tumors.
Related Topics