Chapter: Obstetrics and Gynecology: Ovarian and Adnexal Disease
Benign Ovarian Neoplasms
BENIGN OVARIAN NEOPLASMS
Although
most ovarian enlargements in the reproductive-age group are functional cysts,
about 25% prove to be nonfunctionalovarian
neoplasms. In the reproductive-age group, 90% ofthese
neoplasms are benign, whereas the risk of malignancy rises to approximately 25%
when postmenopausal patients are also included. Thus, ovarian masses in older
patients and in reproductive patients who show no response to oral
con-traceptive treatment are of special concern. Unfortunately, unless the mass
is particularly large or becomes symp-tomatic, these masses may remain
undetected for some time. Many ovarian neoplasms are first discovered at the
time of routine pelvic examination.
Ovarian neoplasms are usually
categorized by the cell type of origin:
·
Epithelial
cell tumors, the largest class of ovarian neo-plasm
·
Germ cell
tumors, which include the most commonovarian neoplasm in reproductive-age
women, the benign cystic teratoma or dermoid
·
Stromal
cell tumors
The classification of ovarian
tumors by cell line of origin is presented in Box 46.1.
Benign Epithelial Cell Neoplasms
The exact
cell source for the development of epithelial
cell tumors of the ovary is unclear; however, the cells are characteristic
of typ-ical glandular epithelial cells. Evidence
exists to suggest thatthese cells are derived from mesothelial cells lining the
peri-toneal cavity. Because the müllerian duct-derived tissue becomes the
female genital tract by differentiation of the mesothelium from the gonadal
ridge, it is hypothesized that these tissues are also capable of
differentiating into glandu-lar tissue. The more common epithelial tumors of
the ovary are grouped into serous, mucinous, and endometrioid neoplasms, as
shown in Box 46.2.
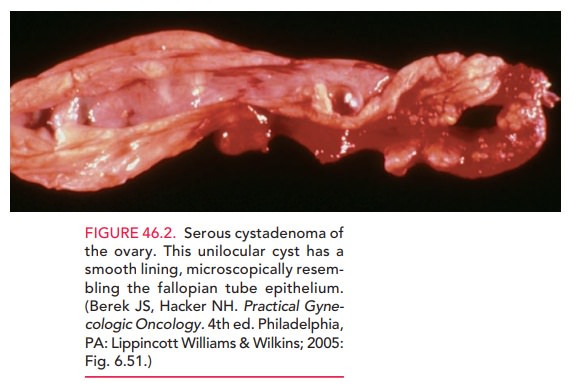
The most common epithelial cell
neoplasm is the serous cystadenoma (Fig.
46.2). Seventy percent of seroustumors are benign; approximately 10% have
intraepithelial cellular characteristics, which suggest that they are of low
malignant potential; and the remaining 20% are frankly malignant by both
histologic criteria and clinical behavior.
Treatment of serous tumors is
surgical, because of the relatively high rate of malignancy. In the younger
patient with smaller tumors, an attempt can be made to perform an ovarian
cystectomy to try to minimize the amount of ovar-ian tissue removed. For large,
unilateral serous tumors in
Box 46.1
Histologic Classification of All Ovarian Neoplasms
From
coelomic epithelium (epithelial)
·
Serous
·
Mucinous
·
Endometrioid
·
Brenner
From
gonadal stroma
·
Granulosa
theca
·
Sertoli–Leydig
(arrhenoblastoma)
·
Lipid
cell fibroma
From
germ cell
·
Dysgerminoma
·
Teratoma
·
Endodermal
sinus (yolk sac)
·
Choriocarcinoma
Miscellaneous
cell line sources
·
Lymphoma
·
Sarcoma
·
Metastatic
·
Colorectal
·
Breast
·
Endometrial
Box 46.2
Histologic Classification of the Common Epithelial Tumors of the Ovary
Serous tumors
Serous
cystadenomas
Serous
cystadenomas with proliferating activity of the epithelial cells and nuclear
abnormalities but with no infiltrative destructive growth (low potential
malignancy)
Serous
cystadenocarcinoma
Mucinous tumors
Mucinous
cystadenomas
Mucinous
cystadenomas with proliferating activity of the epithelial cells and nuclear
abnormalities but with no infiltrative destructive growth (low potential
malignancy)
Mucinous
cystadenocarcinoma
Endometrioid tumors (similar to adenocarcinomas in the endometrium)
Endometrioid
benign cysts
Endometrioid
tumors with proliferating activity of the epithelial cells and nuclear
abnormalities but with no infiltrative destructive growth (low potential
malignancy)
Adenocarcinoma
Brenner tumor
Unclassified carcinoma
young patients, unilateral
oophorectomy with preservation of the contralateral ovary is indicated to
maintain fertility. In patients past reproductive age, bilateral oophorectomy
along with hysterectomy may be indicated, not only because of the chance of
future malignancy, but because of the increased risk of a similar occurrence in
the con-tralateral ovary.
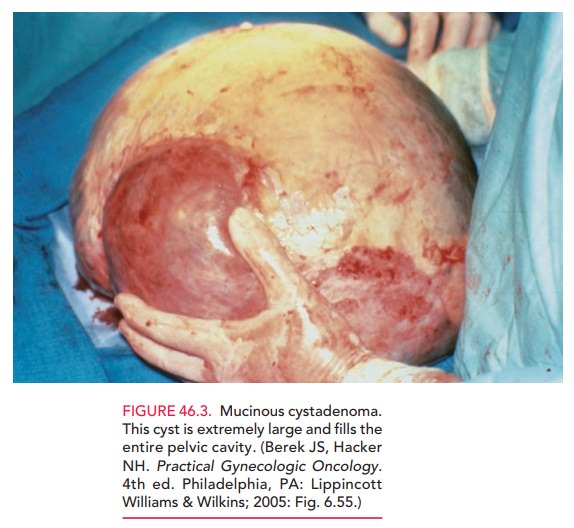
The mucinous cystadenoma is the second most common epithelial cell tumor of the ovary. The malig-nancy rate of 15% is lower than that for serous tumors. These cystic tumors can become large, sometimes filling the entire pelvis and extending into the abdominal cavity (Fig. 46.3). Ultrasound assessment will often reveal multi-locular septations. Surgery is the treatment of choice.
A third type of benign epithelial
neoplasm is the endometrioid tumor. Most
benign endometrioid tumorstake the form of endometriomas, which are cysts lined
by well-differentiated, endometrial-like glandular tissue. For further
discussion of this neoplasm, see “Malignant Ovarian Neoplasms,” later.
The Brenner cell tumor is an uncommon benign epithelial cell tumor of
the ovary. This tumor is usually described as a solid ovarian tumor because of
the large amount of stroma and fibrotic tissue that surrounds the epithelial
cells. It is more common in older women, and occasionally occurs in association
with mucinous tumors of the ovary. When discovered as an isolated tumor of the
ovary, it is relatively small compared with the large size often attained by
the serous and especially by the mucinous cystadenomas. It is rarely malignant.
Benign Germ Cell Neoplasms
Germ cell
tumors are derived from the primary germ cells. Thetumors
arise in the ovary and may contain relatively differ-entiated structures, such
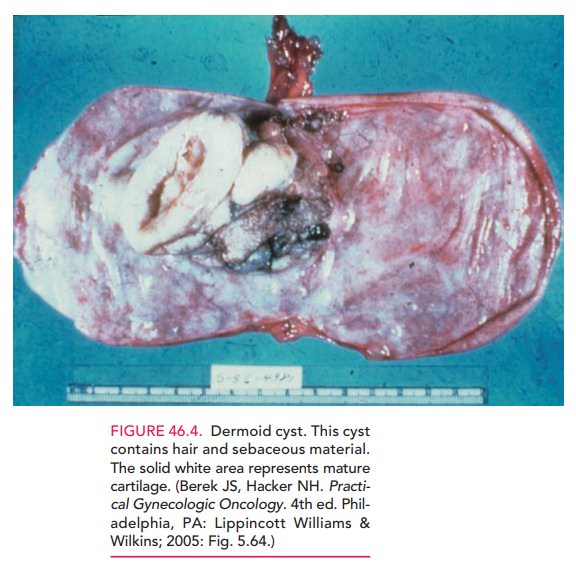
as hair or bone. The most common tumor found in women of all ages is the benign cystic ter-atoma, also called a dermoid cyst or dermoid (Fig. 46.4).Eighty percent occur during the reproductive
years, with a median age of occurrence of 30 years. However, in children and
adolescents, mature cystic teratomas account for about one-half of benign
ovarian neoplasms. Dermoids may contain differentiated tissue from all three
embryonic germ layers (ectoderm, mesoderm, and endoderm). The most common
elements found are of ectodermal origin, primar-ily squamous cell tissue such
as skin appendages (sweat, seba-ceous glands) with associated hair follicles
and sebum. It is because of this predominance of dermoid derivatives that the
term “dermoid” is used. Other constituents of dermoids include central nervous
system tissue, cartilage, bone, teeth, and intestinal glandular elements, most
of which are found in well-differentiated form. One unusual variant is the
struma ovarii, in which functioning thyroid tissue is found.
A dermoid cyst is frequently
encountered as an asymp-tomatic, unilateral cystic adnexal mass that is mobile
and
This tumor often has a
high fat content that makes it more readily identified by computer tomography
(CT) evaluation, as well as giving it a more buoyant ten-dency in the pelvis,
resulting in a relatively high rate of ovarian torsion (15%), in comparison
with other types of neoplasms.
Treatment of benign cystic teratomas is necessarily sur-gical, even though the rate of malignancy is <1%. Surgical removal is required because of the possibility of ovarian tor-sion and rupture, resulting in intense chemical peritonitis and a potential surgical emergency. Between 10% and 20% of these cysts are bilateral, underscoring the need for exam-ination of the contralateral ovary at the time of surgery.
Benign Stromal Cell Neoplasms
Stromal
cell tumors of the ovary are usually considered solid tumors and are derived
from specialized sex cord stroma of the developing gonad. These
tumors may develop along a pri-marily female cell type into granulosa theca cell tumors, or into a
primarily male gonadal type of tissue, known as Sertoli–Leydig cell tumors. Both of these tumors arereferred to as
functioning tumors because of their hormone production. Granulosa theca cell tumors primarily produceestrogenic components and
may be manifest in patients through feminizing characteristics, and
Sertoli–Leydig cell tumors produce androgenic components, which may contribute
to hirsutism or vir-ilizing symptoms. These neoplasms occur with
approximately
When the granulosa cell tumor occurs in
the pedi-atric age group, it may contribute to signs and symptoms of precocious
puberty, including precocious thelarche and vaginal bleeding. Vaginal bleeding
may also occur when this tumor develops in the postmenopausal years. Both the
granulosa cell tumor and the Sertoli–Leydig cell tumor have malignant
potential, as discussed later.
The ovarian fibroma is the result of collagen produc-tion by spindle
cells. These tumors account for 4% of ovarian tumors and are most common during
middle age. It is unlike other stromal cell tumors in that it does not secrete
sex steroids. It is usually a small, solid tumor with a smooth surface and
occasionally is clinically mis-leading because ascites are present. The
combination of benign ovarian fibroma coupled with ascites and right pleural
effusion has historically been referred to as Meigssyndrome.
The following are the key points
that can be made regarding benign ovarian neoplasms:
·
They are more common than
malignant tumors of the ovary in all age groups.
·
The risk for malignant
transformation increases with increasing age.
·
They warrant surgical treatment
because of their poten-tial for malignancy or torsion.
·
Preoperative assessment may be
assisted by the use of pelvic imaging techniques such as ultrasound.
·
Surgical treatment may be
conservative for benign tumors, especially if future reproduction is desired.
Related Topics