Chapter: Basic Radiology : Plain Film of the Abdomen
Exercises: Pelvic Calcifications
EXERCISES 8-2.
PELVIC CALCIFICATIONS
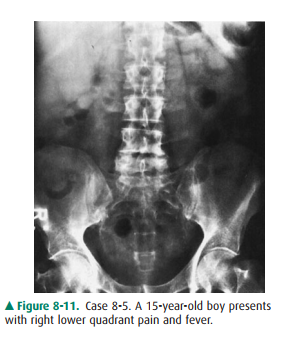
8-5. What is the most
likely diagnosis in Case 8-5 (Figure8-11)?
A.
Appendicolith
B.
Ectopic gallstone
C.
Pelvic phlebolith
D.
Right ureteral calculus.
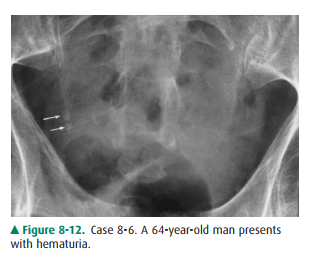
8-6. What is the most
likely diagnosis in Case 8-6 (Figure8-12)?
A.
Calcified ovarian tumor
B.
Multiple phleboliths
C.
Multiple ureteral calculi
D.
Uterine fibroid calcification
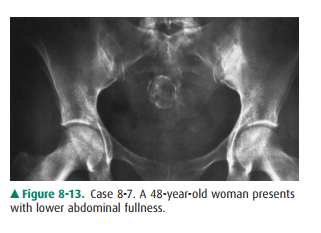
8-7. What is the most
likely diagnosis in Case 8-7 (Figure8-13)?
A.
Bladder calculus
B.
Chondrosarcoma of the sacrum
C.
Cystadenoma of the ovary
D.
Uterine fibroid calcifications
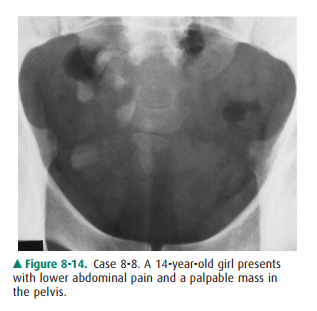
8-8. What is the most
likely diagnosis in Case 8-8 (Figure8-14)?
A.
Bladder calculi
B.
Calcified vas deferens
C.
Ovarian dermoid cyst
D. Uterine fibroid calcification.
Radiologic Findings
8-5. This case is that
of a boy with acute appendicitis (A is the correct answer to Question 8-5). An
oval calcifi-cation measuring 0.8 cm in diameter projects over the iliac bone
and laterally to the right sacroiliac joint with a distended appendiceal lumen
filled with gas. At surgery, gangrenous appendicitis with perforation and an
obstructing appendicolith were found.
8-6. This case
demonstrates 5 5 mm and 4 4 mm cal-cified densities (arrows) along the expected
course of the right distal ureter. These densities were formerly identified in
the right kidney and have migrated infe-riorly to the current position,
indicating right ureteral calculi. With the history of hematuria, the most
likely choice would be right ureteral calculi (C is the correct answer to
Question 8-6).
8-7. This case shows
large, 2-cm-diameter mottled and curvilinear calcifications in the midpelvis.
These cal-cifications overlie the sacrum and are consistent with calcification
in uterine fibroids (D is the correct an-swer to Question 8-7).
8-8. This case shows
several “teeth-like” calcifications in the right side of the pelvis. With a
palpable pelvic mass, the most likely diagnosis is ovarian dermoid cyst. (C is
the correct answer to Question 8-8.)
Discussion
Calcified appendiceal stones are
present in only about 10% of patients with appendicitis; however, in a
symptomatic child, an appendicolith indicates at least a 90% chance ofacute
appendicitis. Prophylactic appendectomy has been recommended in the child with
an incidentally discovered appendicolith because of a high incidence of
gangrene and perforation. CT or ultrasound are better choices in evaluat-ing
appendicitis.
Ureteral calculi are always a consideration
in patients with hematuria. About 50% of urinary calculi are radiographically
opaque and shown on the plain abdominal radiograph. Close scrutiny of the
abdominal film is crucial because ureteral cal-culi may be elusive when they
project over the lumbar trans-verse processes or the sacroiliac region. To
confirm a ureteral calculus, CT is often needed to localize the density to the
ureter. CT is more sensitive in evaluating ureteral calculi. Phleboliths are
thrombi within the pelvic veins, and this loca-tion accounts for their circular
shape. Calcification within these thrombi starts peripherally with a typical
radiolucent center that is seen radiographically. Phleboliths have little
clinical significance except that they can be confused with other pelvic
densities, particularly distal ureteral calculi. In general, ureteral stones
lie above and medially to the ischial spines, and they lack a radiolucent
center.
Most uterine leiomyoma
calcifications appear as multiple mottled or speckled calcifications or as
dense, smooth, curvi-linear calcifications around the mass. The real
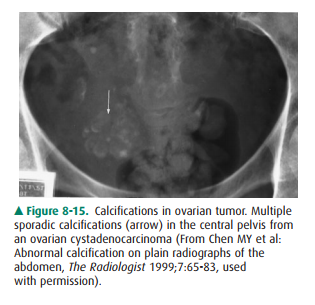
soft-tissue mass is often larger than the area of calcification. Other
calcifications in the pelvis include calcified ovarian tumors (Figure 8-15),
foreign material, lymph nodes, or prostate.
Ovarian dermoid cyst accounts for
about 10% of ovar-ian neoplasms. Ovarian dermoid cyst range from 6 to 15 cm in
diameter and contain teeth, abortive bone, and curvilin-ear capsular
calcification, which may be seen on plain radi-ograph. Dermoid cyst may contain
sebaceous material simulating low-density fat compared to surrounding soft
tissue.
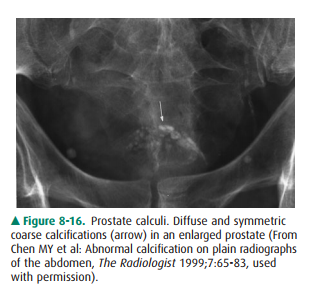
Bladder stone is often seen in
association with bladder outlet obstruction. Bladder calculi are composed of
mixed calcium oxalate and phosphate salts that are radiopaque. Other
calcifications in the bladder include foreign body, transi-tional cell
carcinoma, urachal carcinoma, Schistosoma
infesta-tion, tuberculosis, or alkaline encrusting cystitis. Calcifications in
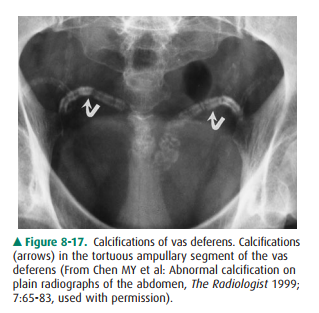
the same area include prostatic calculi (Figure 8-16) and calcified vas
deferens (Figure 8-17). The prostate gland may be calcified. If enlarged, it
may protrude into the bladder.
Related Topics