Chapter: Basic Radiology : Plain Film of the Abdomen
Exercise: Intestinal Distention
EXERCISE 8-4.
INTESTINAL DISTENTION
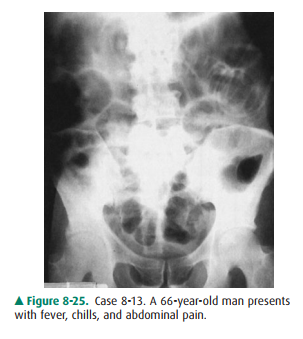
8-13. What is the most likely
diagnosis in Case 8-13 (Figure8-25)?
A.
Functional ileus of the bowel
B.
Mechanical obstruction of the colon
C.
Mechanical obstruction of the small bowel
D.
Pneumoperitoneum
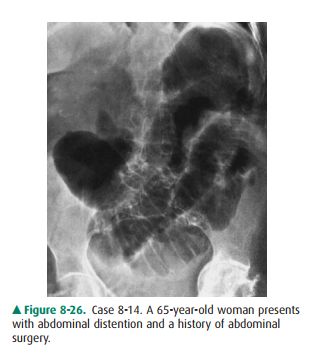
8-14. What is the most
likely diagnosis in Case 8-14 (Figure8-26)?
A.
Functional ileus of the bowel
B.
Gastric outlet obstruction
C.
Mechanical obstruction of the small intestine
D.
Pneumoperitoneum.
8-15. What is the most
likely cause of the distended bowel loop (arrowheads) in Case 8-15 (Figure
8-27)?

A.
Cecal volvulus
B.
Functional ileus of the bowel
C.
Pneumoperitoneum
D.
Sigmoid volvulus.
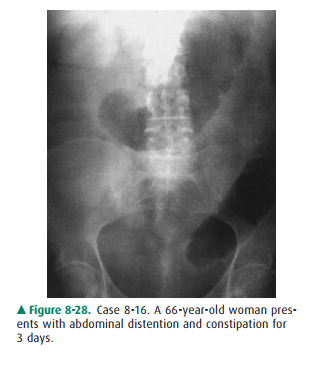
8-16. What is the most
likely diagnosis in Case 8-16 (Figure8-28)?
A.
Ascites
B.
Functional ileus of the bowel
C.
Mechanical obstruction at the colon
D. Mechanical obstruction at the small bowel.
Radiologic Findings
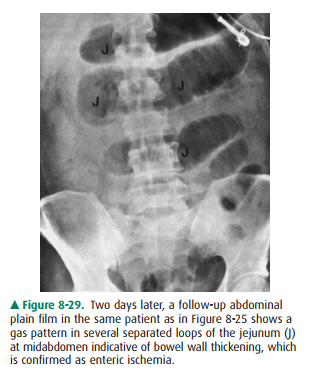
8-13. In this case, a
diffuse abnormal gas pattern with dis-tention of the small bowel, colon, and
rectum sug-gests functional ileus. Two days later the patient underwent
laparotomy, and small-bowel ischemia was found (Figure 8-29) (A is the correct
answer to Question 8-13). Separation of bowel loops may indi-cate bowel wall
thickening but is a nonspecific sign.
8-14. This case shows
gaseous distention of the stomach, duodenum, and jejunum on the supine film,
but no gas is seen in the colon, suggesting mechanical small-bowel obstruction.
Gastric outlet or duode-nal obstruction is unlikely because many jejunal loops
are dilated. At surgery, an obstructing jejunal adhesion was found (C is the
correct answer to Question 8-14).
8-15. This patient has a
huge distended and folded colonic loop in the midabdomen and pelvis (the
“coffee bean” sign). The most likely consideration is a sigmoid volvulus (D is
the correct answer to Question 8-15).
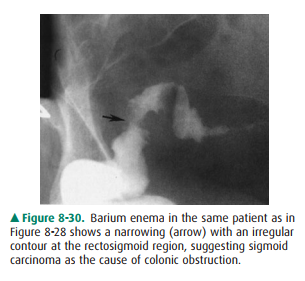
8-16. This case shows
distended transverse colon and de-scending colon and no gas in the sigmoid
colon and rectum. The small bowel is not distended. Mechani-cal obstruction of
the colon distal to the level of de-scending colon is likely (C is the correct
answer to Question 8-16). Barium enema (Figure 8-30) showsan irregular
narrowing at the rectosigmoid region, indicative of sigmoid carcinoma.
Discussion
Generalized or diffuse
distribution of gas, both in the small bowel and in the colon, is more
indicative of a functionalileus. The most common causes of functional ileus are
post-operative status, neuromuscular diseases, ischemia, and in-trinsic or
extrinsic inflammations. Air-fluid levels may be seen in patients with functional
ileus when plain films are ob-tained with the patient in upright or decubitus
position.
Limited distribution of abnormal
gas in the intestine fa-vors a mechanical obstruction. Air-fluid levels may
also be seen in patients with mechanical obstruction when an up-right abdominal
radiograph is obtained. The most com-mon causes of mechanical obstruction in
the small bowel are adhesions, internal or external hernias, neoplasms, or
intussusceptions. Ileocolic intussusception is common in children.
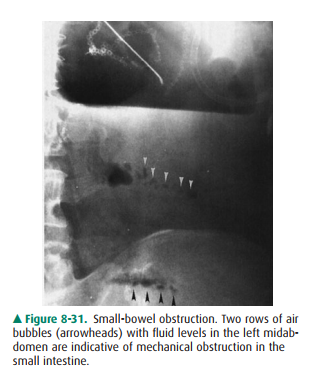
When the small bowel is filled
with a large amount of fluid, a row of small gas bubbles may be trapped between
the valvulae conniventes. The row of gas bubbles is called the “string of
beads” or “string of pearls” sign and is seen on the decubitus or upright view
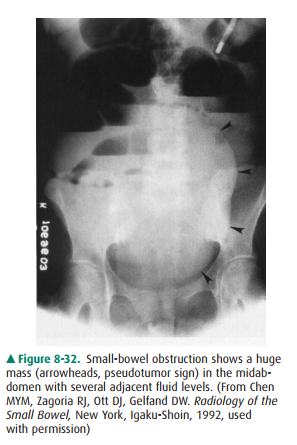
of the abdomen (Figure 8-31). A fluid-filled, closed-loop small bowel
obstruction may appear as an oval mass in the abdomen and is known as the
“pseudo-tumor sign” (Figure 8-32). These signs suggest a mechanical obstruction
and possible strangulation.
Sigmoid volvulus may twist along
the mesenteric axis and the long axis of the bowel. The twisted and
overdis-tended sigmoid colon may appear as an inverted U shape or a coffee bean
shape, without haustra or septa, at the upperpelvis and abdomen crossing the
transverse colon. The colon above the sigmoid may be distended; however, the
small bowel is rarely distended in a patient with sigmoid volvulus. Barium
enema may show a beaking sign adjacent to the twisted point. Vascular
insufficiency may occur if volvulus cannot be corrected.
A small-bowel volvulus may be
caused by internal hernia or adhesion similar to that of sigmoid volvulus.
Small-bowel volvulus may be located outside the pelvis with no proximal colonic
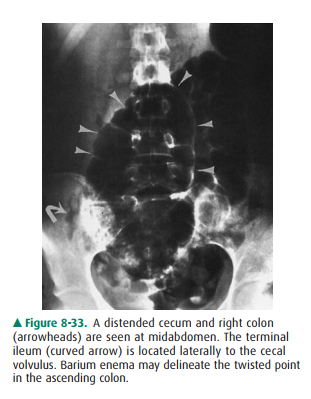
dilatation. Cecal volvulus is the cause of 1% to 2% of intestinal obstructions.
Most often a cecal volvulus is twisted and relocated in the midabdomen or left
upper quadrant (Figure 8-33).
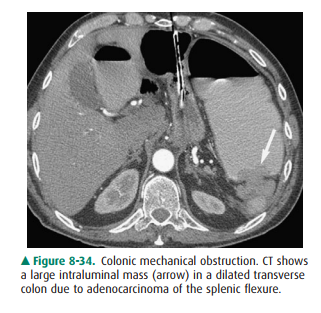
Mechanical obstruction of the
colon is commonly caused by colonic neoplasm, volvulus, or inflammatory mass
caused by diverticulitis of the left colon. All colonic segments proxi-mal to
the mechanical obstruction are distended with gas or a combination of gas and
feces. When intestinal secretions and fecal matter fill the distended bowel
loop, solid and liquid contents produce a mottled appearance. Whether the small
bowel becomes distended from a colonic obstruc-tion depends on its duration and
severity, and also on the competency of the ileocecal valve. Abdominal
radiographs are often of limited value in differentiating the cause of bowel
distention, and CT is more useful for locating a mechanical obstruction (Figure
8-34).
Related Topics