Chapter: Basic Radiology : Plain Film of the Abdomen
Exercise: Upper Abdominal Calcifications
EXERCISE 8-1.
UPPER ABDOMINAL CALCIFICATIONS
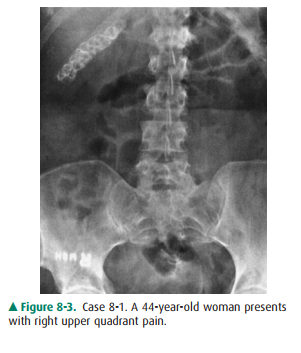
8-1. What is the most
likely diagnosis in Case 8-1 (Figure8-3)?
A.
Adrenal calcification
B.
Calcified gallstones
C.
Kidney stones
D.
Milk-of-calcium bile in the gallbladder
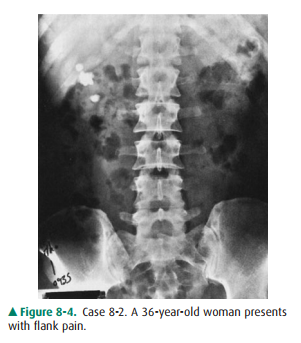
8-2. What is the most
likely diagnosis in Case 8-2 (Figure8-4)?
A.
Adrenal calcification
B.
Calcified gallstones
C.
Kidney stones
D.
Medullary nephrocalcinosis
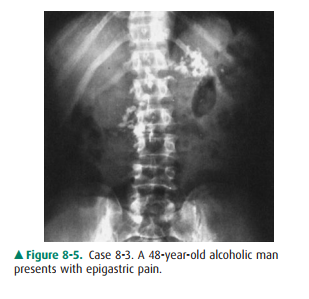
8-3. What is the most
likely diagnosis in Case 8-3 (Figure8-5)?
A.
Adrenal calcification.
B.
Calcified hepatic metastases.
C.
Pancreatic calcification.
D.
Primary calcified mucoproducing adenocarci-noma in the colon.
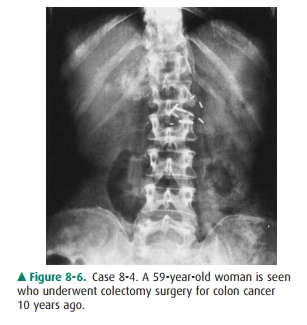
8-4. What is the most
likely diagnosis in Case 8-4 (Figure8-6)?
A.
Adrenal calcification
B.
Calcified hepatic metastases
C.
Pancreatic calcification
D.
Primary calcified mucoproducing adenocarci-
E.
noma in the colon
Radiologic Findings
8-1. This case
demonstrates multiple faceted calcifications in the right upper quadrant that
are characteristic for gallstones (B is the correct answer to Question 8-1).
8-2. This case shows
three separate deposits of calcified density confined to the right renal
shadow. The largest one measures 2 cm in greatest diameter (C is the correct
answer to Question 8-2).
8-3. This case shows
multiple stippled calcifications in the upper abdomen adjacent to the lumbar
spine. In a pa-tient with a history of alcoholism, pancreatic calcifica-tion
from chronic pancreatitis would be the most likely diagnosis (C is the correct
answer to Question 8-3).
8-4. This case shows stippled and discrete calcifications overlying the right twelfth rib, just above the renal outline. When calcification in the lung base, skin, retroperitoneum, pancreas, kidney, and adrenal glands is excluded, hepatic calcification should be considered in a patient with a history of colon cancer (B is the correct answer to Question 8-4).
Discussion
About 15% to 20% of gallstones
are calcified sufficiently to be seen on plain abdominal film. Most gallstones
comprise mixed components, including cholesterol, bile salts, and bil-iary
pigments. Pure cholesterol and pure pigment stones are uncommon. Calcified
gallstones vary in size and shape. Most gallstones have thin, marginal
calcification with central lu-cency and are laminated, faceted, or irregular in
shape. Some gallstones contain gas in their fissures, whether calcified or
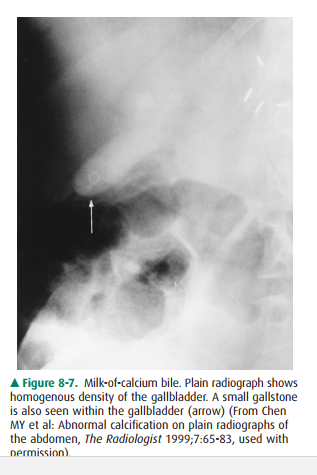
noncalcified. Milk-of-calcium or “limy” bile occurs in pa-tients with
long-standing cystic duct obstruction. The bile contains a high concentration
of calcium carbonate and is densely radiopaque on plain radiograph (Figure
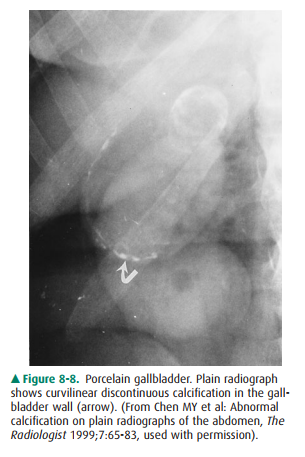
8-7). Calcifi-cation of the gallbladder wall (porcelain gallbladder) devel-ops
in patients with chronic cholecystitis, cholelithiasis, and cystic duct
obstruction. Porcelain gallbladder is characterized by curvilinear calcification
in the muscular layer of the gall-bladder mimicking a calcified cyst (Figure
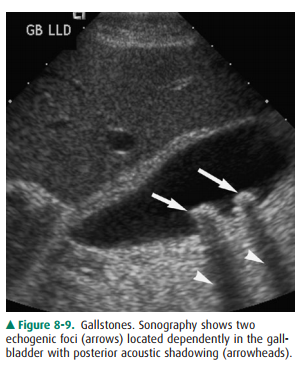
8-8). In general, ultrasonography is the primary modality now used to evalu-ate
the gallbladder (Figure 8-9).
Nephrolithiasis is the most
common cause of calcification within the kidneys. Most renal calculi (85%)
contain calcium complexed with oxalate and phosphate salts. Any process that
creates urinary tract stasis may cause the development of uri-nary calculi.
Renal calculi are usually small and lie within the pelvicalyceal system or in a
calyceal diverticulum. They may remain and increase in size, or they may pass
distally. When calcifications are seen projecting over the renal shadows on
routine films of the abdomen, an oblique view may be obtained to localize the
densities in relation to the kidneys. A staghorn calculus contains calcium
mixed with magnesium, ammo-nium, and phosphate and forms in the environment of
recur-rent urinary tract infection with alkaline urine. CT is more sensitive
than plain radiography in evaluating urinary calculi.
The adrenal gland is located at
the superomedial part of the adjacent kidney. The right gland is lower than the
left.
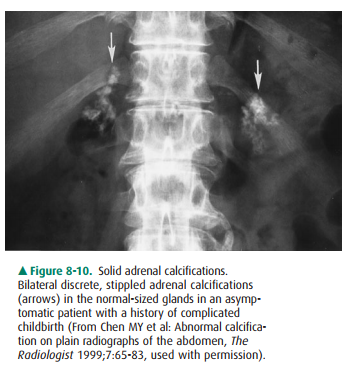
Normally the adrenal gland
measures less than 2.5 3 cm. Stippled, mottled, discrete, or homogeneous
calcifications may appear as a portion of the adrenal gland or may occupy the
entire organ, forming a triangular clump in the adrenal glands (Figure 8-10).
Most adrenal calcifications are inciden-tal findings in normal-sized glands.
They are caused by neonatal adrenal hemorrhage, prolonged hypoxia, severe
neonatal infection, or birth trauma. Less than one-fourth of patients with
Addison’s disease have adrenal calcifications.
In the United States, 85% to 90%
of patients with pancreatic lithiasis are alcoholics. Conversely, less than
half of patients with chronic pancreatitis ever develop pancreatic
calcifications visi-ble on plain radiograph. Although gallstones passing
through the biliary tract can cause acute pancreatitis, chronic pancreati-tis
or pancreatic calcification is rarely caused by cholelithiasis.
Hepatic calcifications are caused
primarily by neoplasms, infections, or parasitic infestations. Primary hepatic
tumors, both benign and malignant, may have calcifications. Colonic carcinoma
and papillary serous cystadenocarcinoma of the ovary are the most frequent
primary tumors causing calcified metastases in the liver. Other primary
neoplasms in the thyroid gland, lung, pancreas, adrenal gland, stomach, kidney,
and breast may cause calcified hepatic metastases. Inflammatory calcified
granulomas related to tuberculosis or histoplasmosis are common in miliary
calcifications. Calcified cystic lesions, such as Echinococcus disease in the liver, are commonly seen in areas of
the world where the causative organism is endemic.
Related Topics