Chapter: Basic Radiology : Imaging of the Spine
Exercise: Spine Trauma
EXERCISE 13-3.
SPINE TRAUMA
13-8. What
is the most
likely diagnosis in
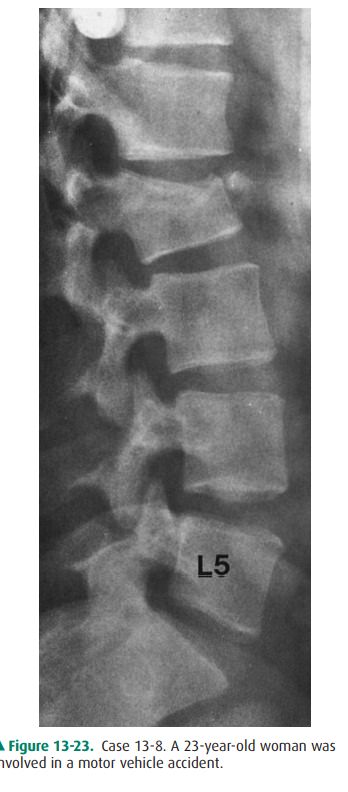
Case 13-8(Figure 13-23)?
A.
Abnormality of bone density
B.
Disruption of facet joints at multiple levels
C.
Subluxation of L4 over L5
D.
12 compression fracture with kyphotic angulation
13-9. Regarding the
patient in Case
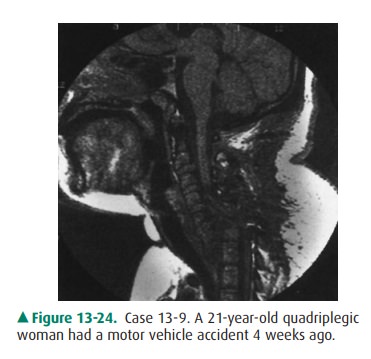
13-9 shown in Figure 13-24, which of the following is
true?
A.
The condition probably predated the trauma.
B.
The prospects for a full recovery are good.
C.
Surgical repair will likely be successful.
D.
The patient will probably never have normal
E.
The spinal cord is intact.
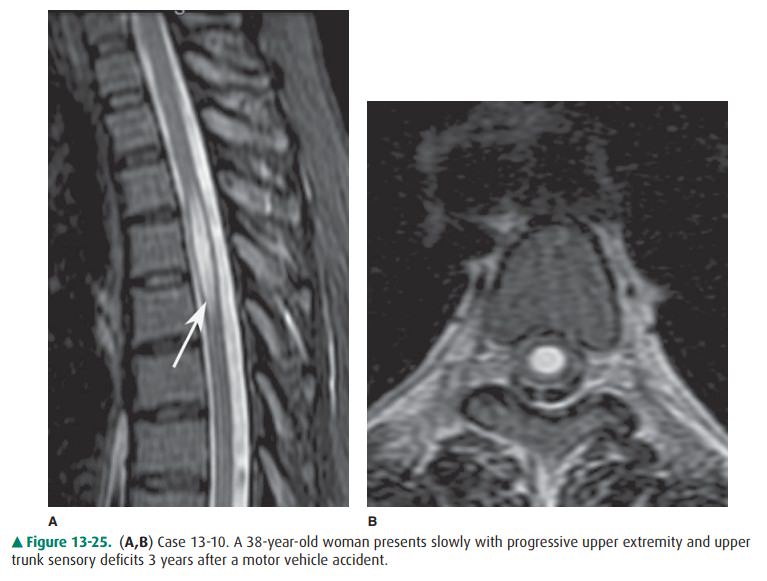
13-10. In Case 13-10, the MRI in Figure 13-25 most likely demonstrates delayed posttraumatic syrinx.
A.
subluxation.
B.
spinal cord tumor.
C.
abnormal bone marrow
Radiologic Findings
13-8. In this case, there is a compression fracture of the L2
vertebral body with kyphotic angulation (E is the correct answer to Question
13-8).
13-9. In this case, the sagittal T1-weighted MR image shows a
complete subluxation of C6 on C7 and a complete transection of the cervical
spinal cord at that level. In all likelihood this patient will never regain use
of her legs or have any normal neurologic function below C6 (D is the correct
answer to Question 13-9).
13-10. In this case, the sagittal T2-weighted MR image shows a
high signal abnormality (arrow) within the upper thoracic spinal cord, and on
the axial T2-weighted image, an epicenter in the central canal region is
con-firmed. This is a typical appearance of syringomyelia or syrinx (A is the
correct answer to Question 13-10).
Discussion
Spinal trauma is a major medical
problem, usually caused by motor vehicle and occupational accidents. Accurate
and complete diagnosis is essential to maintain spine stability and ensure
preservation of neurologic function. As mentioned previously, plain films are
commonly obtained initially. How-ever, additional imaging tests are often
necessary to fully eval-uate a case of spine trauma, especially in high-risk
injury cases, patients with clinical signs and symptoms, or those with altered
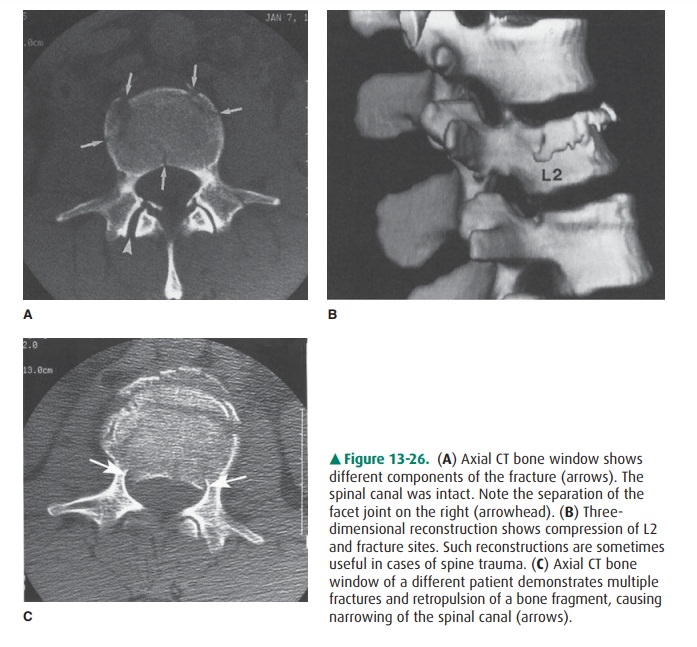
cognition. In Case 13-8, there was clinical con-cern that the spinal canal was
compromised. Small bony frag-ments within the spinal canal may not be visible
with plain film alone. For this reason, CT was performed (Figures 13-26 A, B).
This allowed a better appreciation of the extent of the fractures and ruled out
neural compression. An example of spinal canal compromise is shown in Figure
13-26 C.
In severe trauma, the spinal cord
may be affected. Contu-sions may occur with or without fracture/subluxation,
and MR imaging would be required for diagnosis. In a severe
fracture/subluxation, the spinal cord can be completely tran-sected. In Case
13-9, the patient was known to have a severe C6-7 subluxation, but because of
obesity, plain film and CT imaging were very limited. In this case, only MR
imaging was able to demonstrate the full extent of her spinal cord injury.
Rarely, patients who have
recovered from an acute spinal injury experience a delayed onset of neurologic
symptoms, occurring 1 to 15 years after the trauma. This suggests the
possibility of delayed posttraumatic syrinx (Case 13-10). Symptoms include pain
on coughing or exertion, sensory disturbances, or motor deficits. MR imaging is
essential for diagnosis. The condition is sometimes amenable to surgical
shunting. Syringomyelia can also be idiopathic or can be sec-ondary to certain
congenital or inflammatory conditions. Imaging often cannot distinguish among
different possible etiologies, and history is important.
Related Topics