Chapter: Basic Radiology : Imaging of the Spine
Exercise: Degenerative Spine Disease
EXERCISE 13-1.
DEGENERATIVE SPINE DISEASE
13-1. What is the abnormality in Case 13-1 (Figure 13-9)?

A.
The bones are too dense.
B.
The bones are not dense enough (osteopenia).
C.
There is a destructive bony lesion.
D.
There is an abnormality of alignment.
E.
There is a soft-tissue abnormality.
13-2. In Case 13-2, the lesion represented by an arrow in
Figure 13-10 is most likely to be

A.
a right-sided L4-5 herniated nucleus pulposus.
B.
an extradural tumor.
C.
an epidural abscess.
D.
an intradural mass.
E.
a bony lesion.
13-3. In Case 13-3, the lateral cervical spine plain film in
Figure 13-11 suggests that the most
likely diagnosis is

A.
degenerative disk disease at C2-3 and C3-4.
B.
neoplastic disease at C4.
C.
degenerative disk disease at C5-6 and C6-7.
D.
traumatic injury.
E. disk space infection at C5-6 and C6-7.
Radiologic Findings
13-1. In this case, there is subtle anterior displacement of
the L5 vertebral body relative to S1, known as spondylolis-thesis (D is the
correct answer to Question 13-1).
13-2. In this case, an extradural defect is seen at and below
the L4-5 disk space, and the right L5 nerve root does not fill. These changes
are most likely caused by a disk herniation (A is the correct answer to
Question 13-2). Note the nor-mal filling of the right L4 nerve root
(arrowheads).
13-3. In this case, there is disk space narrowing, and
osteo-phytes are seen at the C5-6 and C6-7 disk spaces (C is the correct answer
to Question 13-3).
Discussion
Degenerative osteoarthropathy may
affect different parts of the spine. When the facet joints are involved, the
result is often bonyosteophytes, which may project into the neural foramen or
spinal canal and compress neural structures. When the disk space is affected,
bony changes in the vertebral body endplate can occur. In addition, the
intervertebral disk itself may be af-fected, and disk herniation can occur as a
result. Differentiation between disk bulge (generalized extension of the disk,
less than 3 mm beyond the edges of the apophyses, with no significant
compression of cord or thecal sac) and herniation (protrusion or extrusion,
with possible compression of nerves or thecal sac) is not always possible.
Treatment decisions must be based on clinical as well as radiologic data.
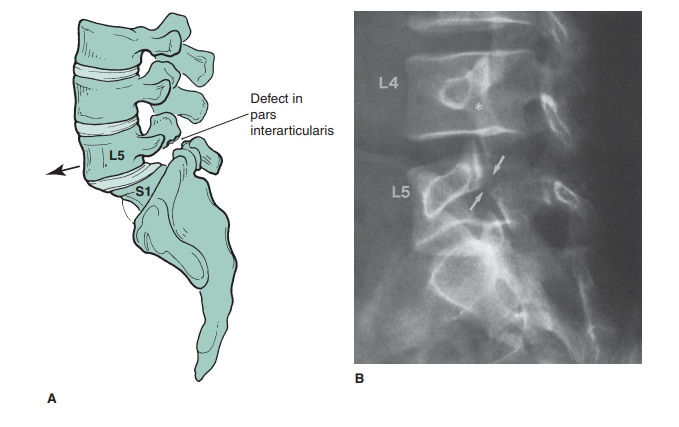
In Case 13-1 (author’s spine),
the spondylolisthesis of L5 over S1 is a result of a defect in the pars
interarticularis. This is the junction of the superior and inferior articular
facet of a given vertebra (Figures 13-3 C and 13-12 A). Spondylolysis, as this
defect is known, is usually caused by a chronic stress fracture, though rarely
it can be congenital or acute. If, as is commonly the case, the spondylolysis
is bilateral, the vertebral body is essentially disconnected from the posterior
elements, and this allows the anterior slipping, or spondylolisthesis, shown in
Figure 13-9. This entity is included here because it is quite common and
predisposes to premature degenerative disease. In older patients,
spondylolisthesis can be secondary to degenerative disease in the absence of a
pars defect, and this “nonlytic” form is known as pseudospondylolisthesis or
degenerative spondylolisthesis. When present, the spondylol-ysis defect is
readily identified on oblique lumbar plain films, as a “broken neck on the
Scottie dog” (Figure 13-12 B). The lysis defect is also readily detected on CT
(Figure 13-12 C), al-though it may superficially resemble a facet joint.
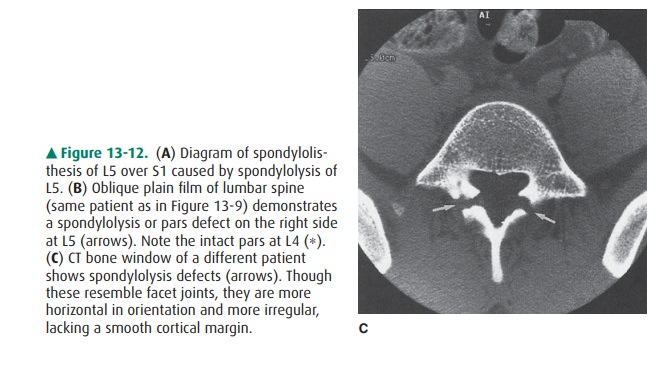
Disk herniations are a common
medical problem. Though they can usually be diagnosed with noninvasive CT or MR
im-aging, myelography is still employed in some places to diag-nose disk
herniations. In Case 13-2, Figure 13-10 shows an extradural defect, seen as an
area of low density distorting the lateral aspect of the thecal sac, deviating
the nerve roots. This is the typical appearance of a herniated nucleus pulposus
(HNP) on myelography. We see the effect of the herniated disk rather than
visualizing the actual disk abnormality. On a CT study, the herniated disk can
also be visualized (Figure 13-13 A). Most of the myelographic filling defect
can be seen to be below the L4-5 disk space, secondary to inferior migration of
disk material. This helps explain why the patient had an L5 radicu-lopathy. The
right L4 nerve root (arrowheads in Figure 13-10) had already exited and would
be unaffected by an L4-5 HNP unless it was far lateral (Figure 13-13 B). As
previously men-tioned, MR imaging is excellent in detecting disk herniations
(Figures 13-13 B, C) and eliminates the need for painful, inva-sive procedures
such as myelography.
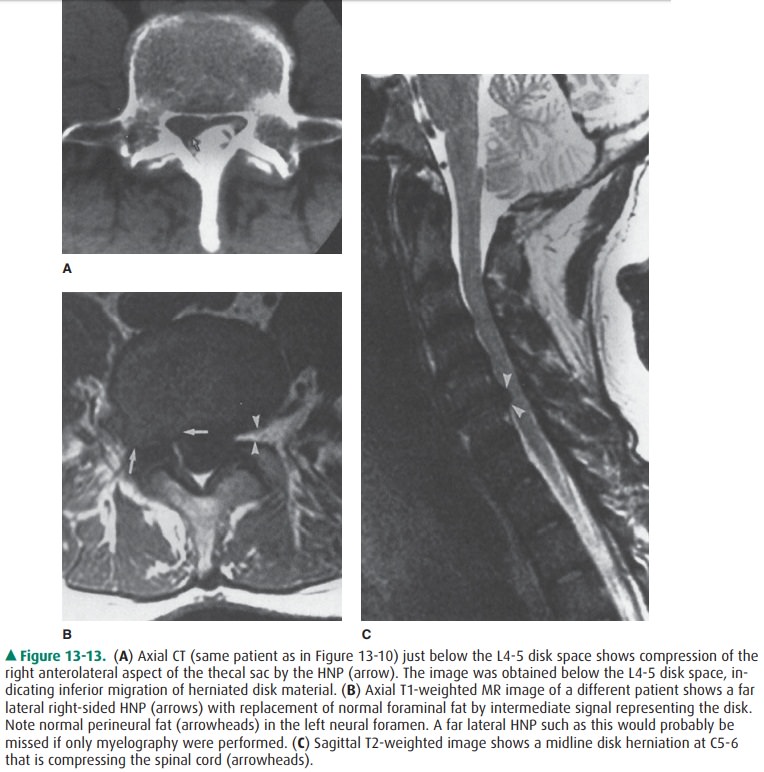
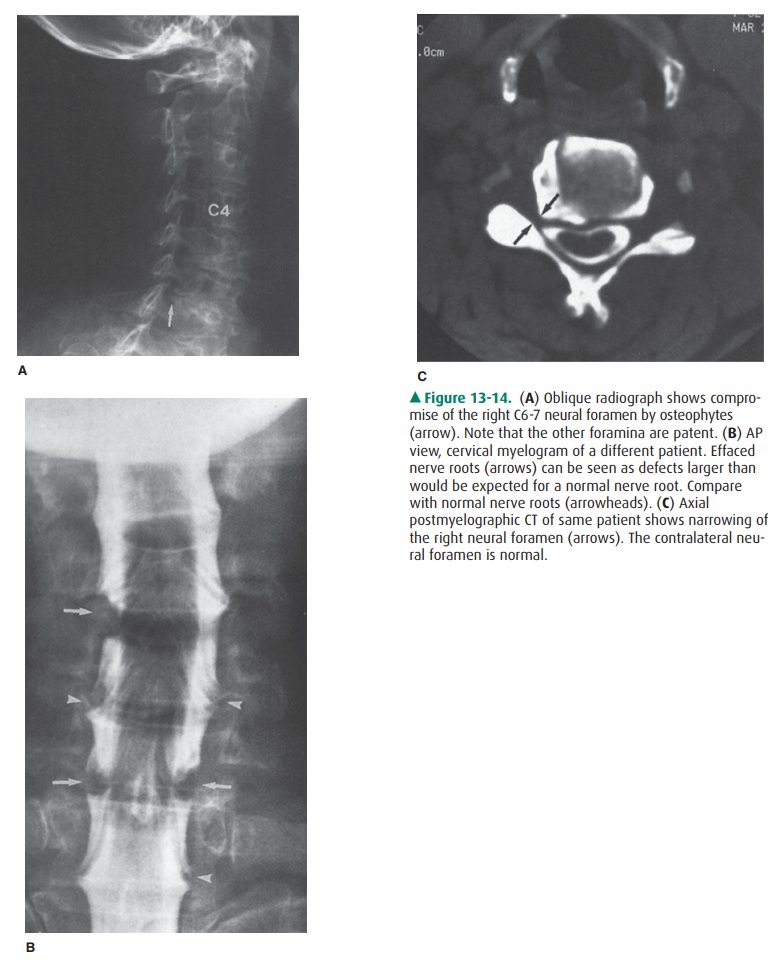
Osteophytic ridging is a common
manifestation of degener-ative bone disease and in the cervical spine may cause
myelopa-thy (if the cord is compressed) or radiculopathy (if a nerve root is
compressed). In Case 13-3, Figure 13-11 shows marked nar-rowing and osteophyte
formation at C5-6 and C6-7. An oblique radiograph is useful in identifying the
foraminal compromise that can result if osteophytes occur in that location
(Figure 13-14 A). Myelography can demonstrate effacement of nerve roots(Figure
13-14 B). CT, with or without intrathecal contrast ma terial, is excellent in
depicting foraminal stenosis caused by osteophytes (Figure 13-14 C). MR imaging
may be limited in its ability to depict subtle bony abnormalities, although
utilization of newer high-resolution sequences have resulted in improved
detection of foraminal stenosis.
Related Topics