Chapter: Basic Radiology : Imaging of Joints
Exercise: Joint Trauma
EXERCISE 7-2.
JOINT TRAUMA
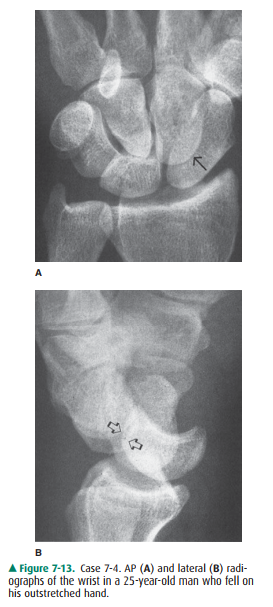
7-4. In Case 7-4 (Figure
7-13), the most likely diagnosis is
A.
lunate dislocation.
B.
perilunate dislocation.
C.
transcaphoid fracture-dislocation.
D.
distal radius fracture.
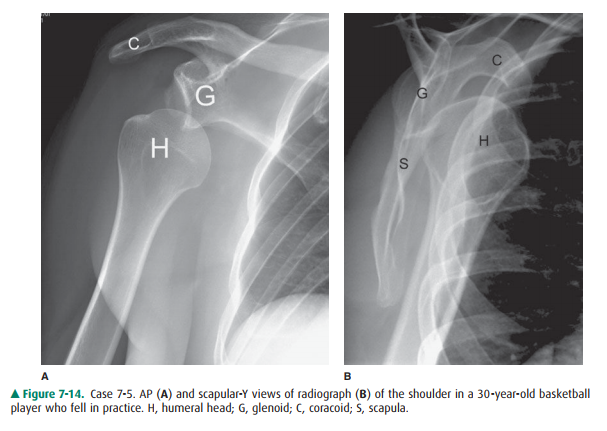
7-5. The basketball
player in Case 7-5 (Figure 7-14) shows which of the following injuries?
A.
Fracture
B.
Dislocation
C.
Osteoarthritis
D.
None of the above
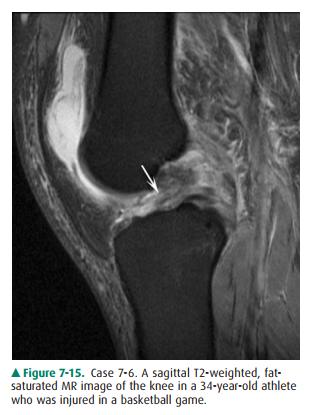
7-6. The basketball
player in Case 7-6 (Figure 7-15) has which type of abnormality on the MR image?
A.
Tendon injury
B.
Muscle injury
C.
Ligament injury
D.
Cartilage injury
7-7. The MR image in
Case 7-7 (Figure 7-16) shows which abnormality?

A.
Muscle injury
B.
Ligament injury
C.
Tendon injury
D.
Cartilage injury
Radiologic Findings
7-4. In the frontal
projection (Figure 7-13 A), there is dis-organization of the carpal arcs. The
capitate is no longer articulating with the lunate and partly over-laps the
scaphoid (arrow). The scaphoid is elongated on this view but not fractured. On
the lateral projec-tion (Figure 7-13 B) the lunate is still in line with the
distal radius, but the capitate has been dislocated dorsally (open arrows).
Therefore, the patient has a dorsal perilunate dislocation (B is the correct
answer to Question 7-4).
7-5. The AP radiograph
of the shoulder of a basketball player (Figure 7-14 A) shows inferior
displacement of the humeral head out of its normal position within the glenoid.
The scapular-Y view of the shoulder (Figure 7-14 B) shows that the humeral head
(H) is dislocated anteriorly in relation to the glenoid (G), thus representing
an anterior shoulder dislocation. S, scapula; C, coracoid. This is the classic
appearance of an anterior dislocation of the shoulder. (B is the cor-rect
answer to Question 7-5.)
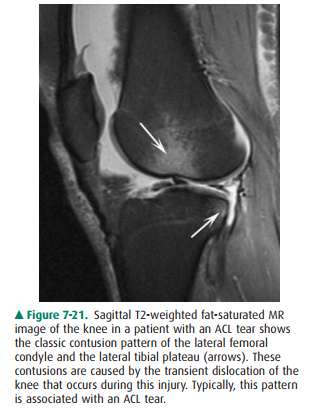
7-6. The sagittal MR
image shows the advantage of MR imaging in this clinical setting. Figure 7-15
shows a tear of the anterior cruciate ligament (ACL) (arrow) (C is the correct
answer to Question 7-6).
7-7. Figure 7-16 shows
the ends of a torn supraspinatus tendon (arrows) in the squash player (C is the
correct answer to Question 7-7).
Discussion
Dislocation or subluxation: The
terms subluxation and dis-location are often used interchangeably. However, subluxa-tion refers to partial loss of
congruity between the articulating
ends of bones, whereas dislocation
denotes com-plete loss of congruity. Disruption or loss of the integrity ofthe
restraining ligaments around the joint leads to insta-bility and thus permits
dislocation to occur. Severe hyper-flexion or hyperextension forces often cause
traumatic dislocations. Fractures are frequently associated with traumatic
dislocations.
Carpal Dislocation
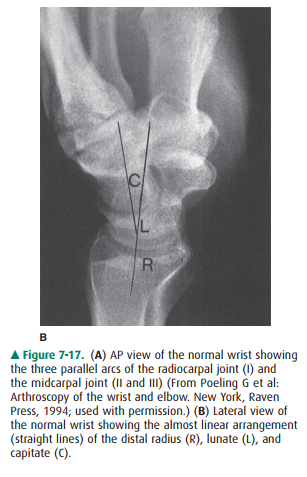
The normal arrangement of the
carpal bones of the wrist is seen on the AP view of the wrist (Figure 7-17 A).
Note the three smooth, parallel arcs in the proximal and mid-carpal rows (arcs
of Gilula). The lateral view of the wrist (Figure 7-17 B) shows that the
radius, lunate, and capitate are in an almost straight line. There are two
major types of wrist carpal dislocation: perilunate and lunate dislocations. In
a perilunate dislocation, the lateral film shows that the lu-nate maintains its
normal articulation with the radius and the capitate is displaced dorsally. In
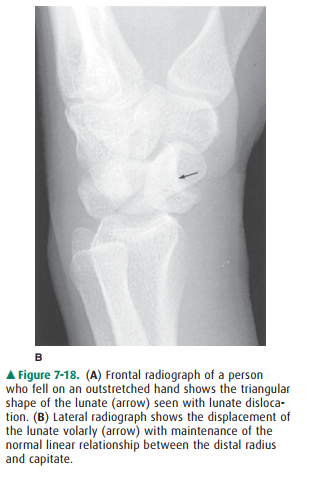
a lunate dislocation, the lunate has a triangular shape on the frontal
projection (Figure 7-18 A) and is displaced from its normal articula-tion and
the radius and capitate maintain a linear relation-ship (Figure 7-18 B). Carpal
dislocations are usually produced by a fall on the outstretched hand (foot) and
are more common common mechanism of injury to the ACL is the “clipping” injury
with valgus stress and internal rotation of the knee. On MR, the injured ACL is
diagnosed by high signal intensity within the substance of the ligament (the
so-called pseudo-mass). There may also be other associated abnormalities such
as bone contusions (usually on the posterolateral aspect of the tibia and the
anterolateral aspect of the femur that result from the transient dislocation
that occurs at the time of in-jury, the so-called kissing contusions) and
medial collateral ligament injury from the valgus stress (Figure 7-21). There
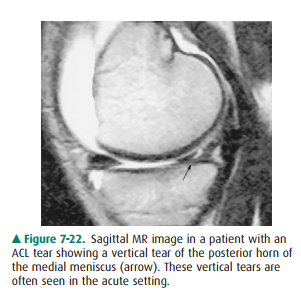
may also be associated meniscal tears, usually vertical tears in the acute
setting (Figure 7-22).


The posterior cruciate ligament
(PCL) serves to limit the posterior translation of the tibia in relation to the
femur. The PCL is commonly injured in kicking sports such as soccer and is also
injured in automobile accidents if the tibia im-pacts on the dashboard and is
translated posteriorly in rela-tion to the femur in a flexed knee.
The normal PCL on MR is a
homogeneous structure that originates from the inner aspect of the medial
femoral condyle and extends far posteriorly to insert onto the poste-rior
aspect of the tibia (Figure 7-23). The PCL should easily be seen on all knee MR
studies. Tears of the PCL are diagnosed using MR imaging. Partial tears are
identified by increased T2in young adults. The diagnosis is usuallymade by
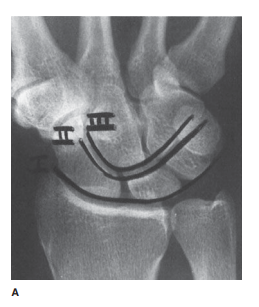
radiographic examination, although CT may be used after reduction to evaluate
the wrist for joint con-gruity and for the presence of intraarticular fracture
frag-ments (“loose bodies”).

Shoulder Dislocation
The two main directions in which
the proximal and humerus dislocates are anterior and posterior. Anterior
dislocation, usually caused by falls, is most common and is seen in about 95%
of cases. In an anterior dislocation, the humeral head is displaced anteriorly
and inferiorly to the scapular glenoid fossa. There are various subtypes of
anterior dislocation: sub-glenoid, subcoracoid, and medial. These subtypes are
based on the location of the humeral head relative to the glenoid fossa and
coracoid process.
Posterior dislocation is relatively
uncommon. It is most commonly associated with severe contraction of the muscles
of the shoulder girdle, which may occur in electric shock or convulsions. A
diagnosis of posterior dislocation in one shoulder should prompt investigation
of the other shoulder, because this injury is often bilateral.
If the postreduction radiographs
are normal after a single instance of dislocation, there is usually no need for
anotherimaging study in the acute setting. However, if there is a re-currence
of dislocation or if the patient remains chronically symptomatic, MR imaging or
CT arthrography of the shoul-der should be obtained to search for the cause of
the disloca-tions and any associated shoulder abnormalities resulting from the
dislocation.
CT arthrography and MR imaging
are used to investigate the shoulder for cartilage and soft-tissue injuries
resulting from shoulder dislocation. After an anterior dislocation, there is
frequently associated injury of the anterior glenoid labrum. This is produced
by impaction of the posterior and lateral aspect of the humeral head against
the anterior and in-ferior portion of the glenoid. There may also be an
accompa-nying compression fracture of the humeral head, referred to as a
Hill-Sachs deformity.
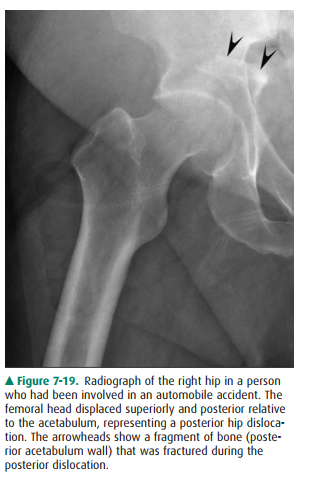
Hip Dislocation
The hip is a relatively stable
joint because of the surrounding strong muscles and joint capsule, and
significant trauma common mechanism of injury to the ACL is the “clipping”
injury with valgus stress and internal rotation of the knee. On MR, the injured
ACL is diagnosed by high signal intensity within the substance of the ligament
(the so-called pseudo-mass). There may also be other associated abnormalities
such as bone contusions (usually on the posterolateral aspect of the tibia and
the anterolateral aspect of the femur that result from the transient
dislocation that occurs at the time of in-jury, the so-called kissing
contusions) and medial collateral ligament injury from the valgus stress
(Figure 7-21). There may also be associated meniscal tears, usually vertical
tears in the acute setting (Figure 7-22).
The posterior cruciate ligament
(PCL) serves to limit the posterior translation of the tibia in relation to the
femur. The PCL is commonly injured in kicking sports such as soccer and is also
injured in automobile accidents if the tibia im-pacts on the dashboard and is
translated posteriorly in rela-tion to the femur in a flexed knee.
The normal PCL on MR is a
homogeneous structure that originates from the inner aspect of the medial
femoral condyle and extends far posteriorly to insert onto the poste-rior
aspect of the tibia (Figure 7-23). The PCL should easily be seen on all knee MR
studies. Tears of the PCL are diagnosed using MR imaging. Partial tears are
identified by increased T2 signal and swelling within the ligament. Complete
tears of the ligament are diagnosed by discontinuity of the ligament fibers at
some point along its course (Figure 7-24). MR imag-ing is extremely important
in the evaluation of the knee of the injured athlete and is used frequently in
this setting.

Supraspinatus Tendon Tears
The supraspinatus, infraspinatus,
teres minor, and subscapu-laris muscles (SITS muscles) comprise the rotator
cuff. De-spite being the most unstable joint in the body, the rotator cuff
muscles help to stabilize the joint. The most commonly torn tendon in the
shoulder is the supraspinatus, and it usu-ally tears approximately 1 centimeter
proximal to its inser-tion onto the anterior aspect of the greater tuberosity
of the humeral head. The supraspinatus tendon is easily seen on MR imaging as a
low-signal-intensity structure, and tears of the supraspinatus tendon are well
demonstrated on MR. The most common causes of supraspinatus tendon tears are aging
and impingement. Acute rotator cuff tears are unusual. MR imaging is vital in
the preoperative evaluation of the patient suspected of having a rotator cuff
tear. The morphology of the tendons, the size of the tear, and other associated
abnor-malities of the joint, including pathology of the glenoid labrum, can be
diagnosed with this technique. Importantly, the degree of muscle atrophy
associated with chronic tears can be assessed, thereby suggesting the
probability of a suc-cessful postoperative recovery and rehabilitation.
Achilles Tendon Rupture
The injury of Achilles tendon
rupture occurs most frequently in patients in the fourth and fifth decades of
life. Althoughthe injury may occur in any person, individuals who do not
exercise regularly (“weekend warriors”) are more susceptible to this tear.
The clinical history and physical
findings are often enough to make a diagnosis of Achilles tendon rupture.
Ra-diographic stress views should not be performed in the set-ting of a
suspected Achilles tendon rupture because the stress may actually make the tear
worse. Any question of whether the tear is partial or complete should be
resolved, as the treatment for each of these is different. Moreover, the
clinician needs to know the level of injury and how far the tendon fragments
are separated. MR imaging is currently the imaging technique of choice to
evaluate the Achilles tendon, although ultrasound is an excellent alternative
and is used more commonly in Europe for this injury. The whole length of the
tendon, including its insertion on the calcaneus, and any associated injuries
can be shown in de-tail. In cases of acute complete rupture of the tendon, the
MR images show discontinuity of the normally low-signal-intensity fibers of the
Achilles tendon, which are replaced by edema and hemorrhage. MRI helps to
quantitate the amount of distraction between the ends of the torn tendon. The
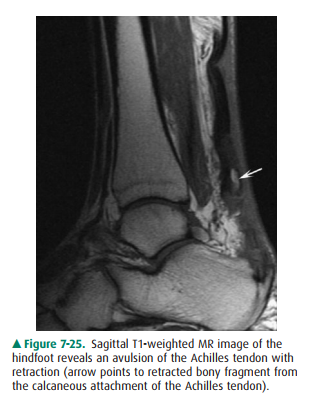
Achilles tendon may also avulse a small portion of bone from its calcaneous
attachment (Figure 7-25). In partial tears, areas of intermediate to high
signal, representing re-gions of partial disruption, are seen within the
normally low-signal-intensity tendon, and some of the fibers of the tendon
remain intact. Ultrasound may also be used to eval-uate the Achilles tendon,
and color Doppler examination may be used to follow the process of
revascularization and healing of a partially torn tendon.
Related Topics