Chapter: Basic Radiology : Imaging of Joints
Exercise: Joint Instability
EXERCISE 7-3.
JOINT INSTABILITY
7-8. The most likely
diagnosis for Case 7-8 (Figure 7-26) is A.
dislocation of the shoulder.

A.
myositis ossificans.
B.
tear of the anterior glenoid labrum.
C.
rotator cuff tear.
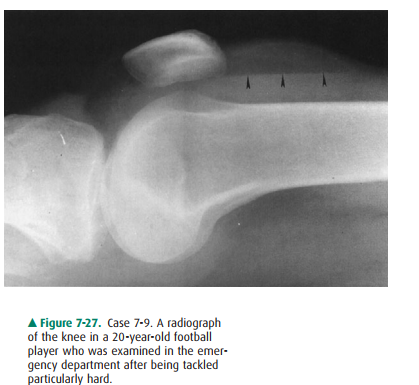
7-9. Regarding Case 7-9
(Figure 7-27), the arrowheads in-dicate a
A.
fracture of the patella.
B.
lipohemarthrosis.
C.
tear of the anterior cruciate ligament.
D.
foreign body.
E.
ligament injury.
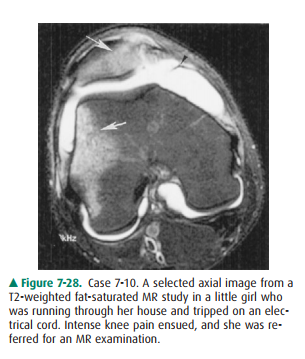
7-10. The axial MR image
for Case 7-10 (Figure 7-28), of a little girl who was injured by tripping on an
electrical cord, shows a
A.
meniscal tear.
B.
tendon injury.
C.
medial retinacular injury.
D.
ligament strain.
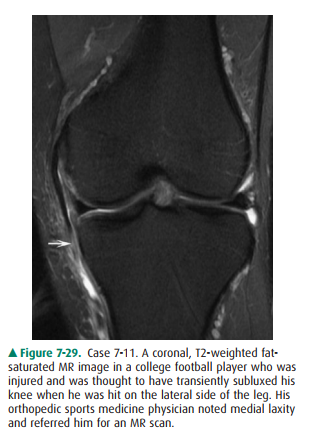
7-11. The medial pain in
the football player in Case 7-11 was most likely caused by (arrow in Figure
7-29)
A.
a medial collateral ligament tear.
B.
a lateral collateral ligament tear.
C.
an anterior cruciate ligament tear.
D. a meniscal tear.
Radiologic Findings
7-8. Figure 7-26 is an axial image. There is a high-signal-intensity line through the triangular anterior glenoid labrum representing an anterior glenoid labral tear (C). (C is the correct answer to Question 7-8.) In Figure 7-26, A is the posterior labrum, B is the biceps tendon, and D is the belly of the subscapu-laris muscle.
7-9. Figure 7-27 is a
lateral radiograph of the knee ob-tained with a horizontal x-ray beam. There is
a joint effusion with a fat-fluid level (arrowheads). This fat-fluid level is
called a lipohemarthrosis. It is important to perform horizontal cross-table
lateral films in the acute trauma setting in order to demonstrate this.
Frequently, there is a fracture to account for the presence of fat within the
joint, as the fat has entered the joint space from the bone marrow cavity (B is
the correct answer to Question 7-9).
7-10. Figure 7-28, the
axial image on the little girl injured by tripping over the electric cord,
shows a large joint effusion and high-signal-intensity areas on the me-dial
aspect of the patella and the lateral aspect of the lateral femoral condyle
(arrows). These are corre-sponding contusions. In this instance, the contusions
result from impingement of the medial aspect of the patella onto the lateral
femoral condyle as the patella dislocates laterally. For this to happen, there
has to be a stretch or tear of the medial retinaculum (arrow-head) (B is the
correct answer to Question 7-10). This constellation of findings is diagnostic
of patellar dislocation-relocation.
7-11. Figure 7-29, a
coronal image of the football player in-jured during a game, shows a complete
tear of the medial collateral ligament (arrow) (A is the correct answer to
Question 7-11). Injuries to the medial side of the knee occur from lateral
trauma (valgus stress). The clinician in this instance noticed the medial joint
laxity and suspected an MCL tear.
Discussion
Instability Disorders
These are functional joint
disorders generally manifested by pain or a sensation of the joint giving way
and abnormal mo-tion around the joint. There may be no radiographic evi-dence
of joint abnormality as often only soft-tissue injuries, such as ligamentous or
fibrocartilaginous tears, are present. These abnormalities can often only be
demonstrated by con-ventional stress views or MR examinations of the joint in
question.
Shoulder Instability
The glenohumeral joint is the
most inherently unstable ball-in-socket joint in the body. The major stability
of the shoulder joint is provided by the joint capsule, the rotator cuff
mus-cles, and the ligaments and tendons that surround it. The gle-noid labrum,
a fibrocartilaginous structure, contributes to shoulder joint stability by
deepening the socket (glenoid labral complex) for this ball (humeral head).
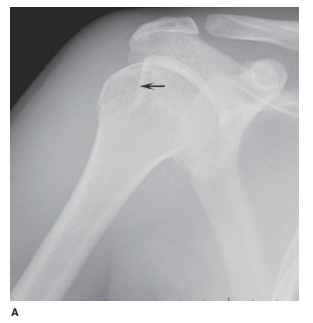
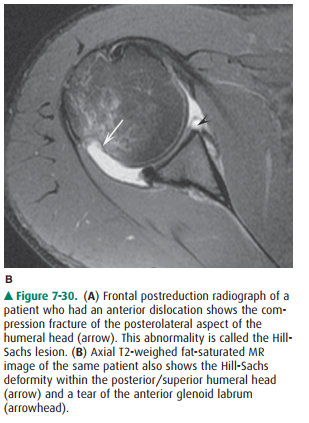
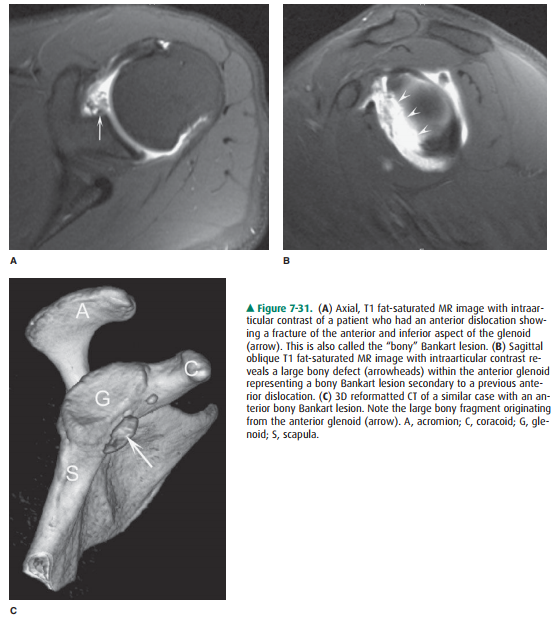
A variety of soft-tissue injuries are associated with
anterior instability syndrome. The most common injuries resulting from anterior
glenohumeral dislocation are an-teroinferior glenoid labral tears (the Bankart
lesion), capsu-lar stripping, Hill-Sachs deformity (compression fracture of the
posterolateral aspect of the humeral head), and glenoid labral tears associated
with osseous fractures (Figures 7-30, 7-31). Tears of the posterior aspect of
the glenoid labrum are seen following posterior dislocation (Figure 7-32). As
we discussed in the last section, ruptures or tears of the ro-tator cuff
tendons (supraspinatus, subscapularis, infra-spinatus, and teres minor [SITS]
muscles) are common causes of shoulder joint dysfunction and instability. The
supraspinatus is the most commonly torn tendon in the shoulder. When the
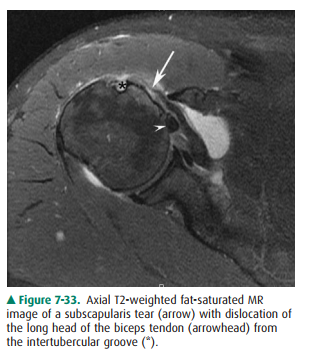
subscapularis tendon tears, there is often an associated dislocation of the
biceps tendon. This results from a tear of the transverse ligament, a fascial
ex-tension across the intertubercular sulcus that holds the bi-ceps in place
(Figure 7-33).

Knee Joint Instability
Stability of the knee, which is a
hinge joint, is provided by the muscles and the ligamentous complexes. The most
im-portant of these are the anterior and posterior cruciate liga-ments and the
lateral and medial collateral ligament complexes. The major knee structures that
cross the joint anteriorly are part of the extensor mechanism, made up of the
quadriceps insertion and the patella ligament. Laterally, the biceps femoris
tendon, tensor fascia lata, and popliteus muscles cross the joint. Medially,
the pes anserinus tendons, which comprise the sartorius, gracilis, and
semitendinosus muscles-(the way to remember this is the phrase, “say grace
before tea”). The gastrocnemius and plantaris muscles are posterior to the
joint. Rupture of any of the tendons, liga-ments, or muscles compromises
stability of the knee joint. All of these structures can be exquisitely
demonstrated with MR imaging, which is the best imaging test to evaluate
insta-bility in this joint.
Related Topics