Chapter: Obstetrics and Gynecology: Disorders of the Breast
Evaluation of Breast Signs and Symptoms
EVALUATION OF BREAST SIGNS AND SYMPTOMS
A timely evaluation of the patient who presents with a breast complaint is important if for no other reason than to relieve patient anxiety. A systematic approach to evalu-ating a breast-related complaint will efficiently yield the proper diagnosis.
The two
most common presenting complaints related to the breast are pain and concern
about a mass. Gynecologistsshould be aware of the different
etiologies of breast pain and be able to offer reassurance, follow-up, and
potential treatment. One study has found that breast cancer was diagnosed in 6%
of patients with breast complaints (most commonly a mass). Therefore, it is important
that breast signs and symptoms be properly evaluated.
Patient History
The patient interview is
considered the single most impor-tant step in the initial evaluation of any
disease process. In the case of complaints related to the breast, questions that
will aid in deciding the next step include the location of complaints, duration
of symptoms, how it was first discov-ered, presence or absence of nipple
discharge, any changes in size, and association with menstrual cycle. In addition, theclinician should ask about
the presence of risk factors that would increase the likelihood of malignancy (Box
31.1).
Physical Examination
A complete breast exam should
evaluate both breasts in a systematic fashion, both axillae, and the entire
chest wall.
The best
time to perform a breast exam is in the follicular phase of the menstrual
cycle.
If the initial exam fails to
yield a dominant mass, the options (based on the patient’s risk factors)
include either performing a repeat exam in 3 months or referral to a spe-cialized
breast care clinic.
Box 31.1
Risk factors for Breast Cancer
·
Age
·
Personal
history of breast cancer
·
History
of atypical hyperplasia (ductal or lobu-lar) on past biopsies
·
Inherited
genetic mutations
·
First-degree
relatives with breast or ovarian cancer diagnosed at an early age
·
Early
menarche (age >12 years)
·
Late
cessation of menses (age >55 years)
·
No
term pregnancies
·
Late
age at first live birth (>30)
·
Never
breastfed
·
Alcohol
consumption
·
Recent
oral contraceptive use
·
Use
of hormone therapy
·
Personal
history of endometrial, ovarian, or colon cancer
·
Jewish
heritage
Diagnostic Testing
After performing a complete
history and physical exami-nation, a number of modalities can be used to help
locate and characterize a breast mass.
MAMMOGRAPHY
Mammography
is an x-ray technique used to study thebreast.
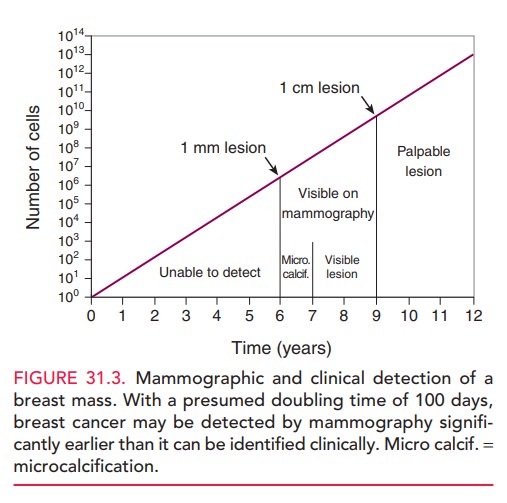
Mammography
is able to detect lesions approximately 2 years before they become palpable
(Fig. 31.3).
Mammography can be done either as
a screening or a diag-nostic test. During a screening mammogram, the patient
stands or sits in front of the x-ray machine. Two smooth plastic plates are
placed around the breast and subsequently compressed to allow for complete
visualization of the tis-sue. A standard
four-image screening mammogram involvestwo craniocaudal and two mediolateral
images. The images areevaluated for defects suspicious of cancer,
microcalcifi-cations, distortion of the normal architecture, and any dis-crete
nonpalpable lesion. Lobular carcinoma is
more difficultto detect with routine screening mammography.
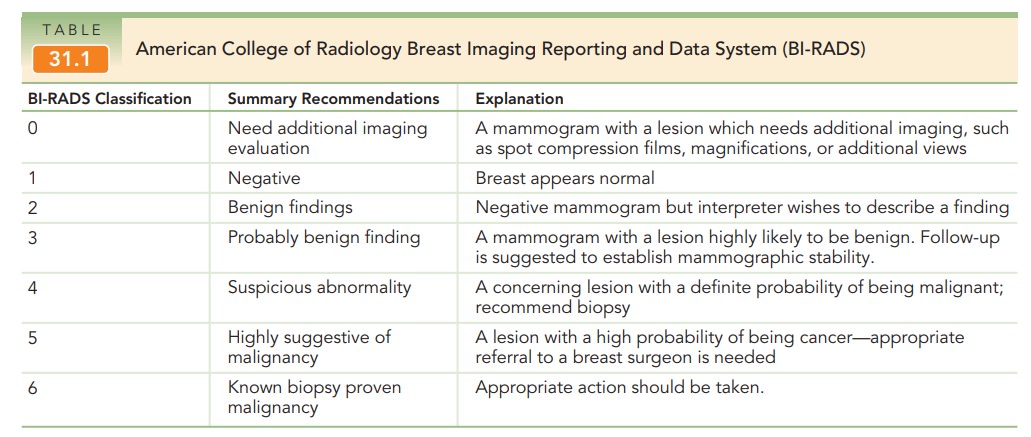
In collaboration with the National Cancer Institute and the FDA, the American College of Radiology has standardized the reporting of mammographic results through a system known as the Breast Imaging Reporting and Data System (BI-RADS®). This system helps clearly communicate the final assessment and recommendations to referring physicians (Table 31.1).
A
diagnostic mammogram is done to supplement an abnor-mal screening mammogram. In women
older than 40 yearsof age, mammography is often used as the first-line study in
evaluating a patient presenting with a breast mass, even if not palpable on
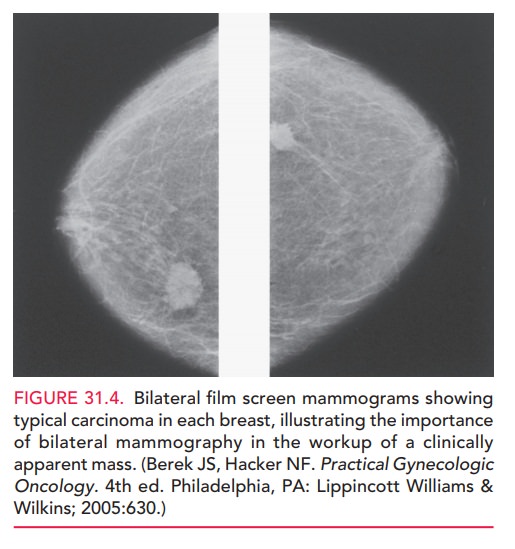
clinical breast examination. Spot com-pressions and magnified views are used to
further localize any lesions, along with providing dimensions of the
surrounding tissue (Fig. 31.4). The
contralateral breastshould also be imaged in cases of a clinically apparent
mass. If possible, the lymph nodes are also imaged to search for unrecog-nized
abnormalities.
ULTRASONOGRAPHY
Ultrasonography has come to play an important role in the evaluation of breast lesions. It is useful in evaluating the breasts of young women and others with dense tissue, differentiating between a solid and cystic mass, and in guiding tissue core-needle biopsies. An anechoic defect found on ultrasound is consistent with a simple cyst and can be drained for symptomatic relief. In women youngerthan 40 years of age, ultrasonography is the recommended ini-tial modality to evaluate a breast mass.
MRI
Magnetic resonance imaging (MRI)
can be a useful adjunct to diagnostic mammography. The use of MRI for screeningthe general population is limited by the
cost of the exam, lack of standard examination technique, and inability to
detect micro-calcifications. However, MRI is being used for early
detec-tion of breast cancer in women at very high risk.
FINE-NEEDLE ASPIRATION BIOPSY (FNAB)
Fine-needle
aspiration is useful in determining if apalpable lump is a
simple cyst. The procedure is per-formed in the office with the aid of local
anesthesia. The sus-pected mass is stabilized between two fingers of one hand
and aspirated using a 22-gauge to 24-gauge nee-dle. Clear aspirated fluid does
not need to undergo pathologic evaluation, and the patient may return for a
clinical breast evaluation within 4 to 6 months if the mass disappears. If it
reappears, the patient is managed with diagnostic mammography and
ultrasonography. Bloody aspirated fluid should be evaluated pathologi-cally,
and the patient should undergo diagnostic mam-mography and ultrasonography.
CORE-NEEDLE BIOPSY
In a core-needle biopsy, a large needle (14 to 16 gauge) is used to
obtain samples from larger, solid breast masses. Three to six samples of tissue
approximately 2 cm long are obtained and are evaluated for abnormal cells in
relation to the surrounding breast tissue taken in the sample.
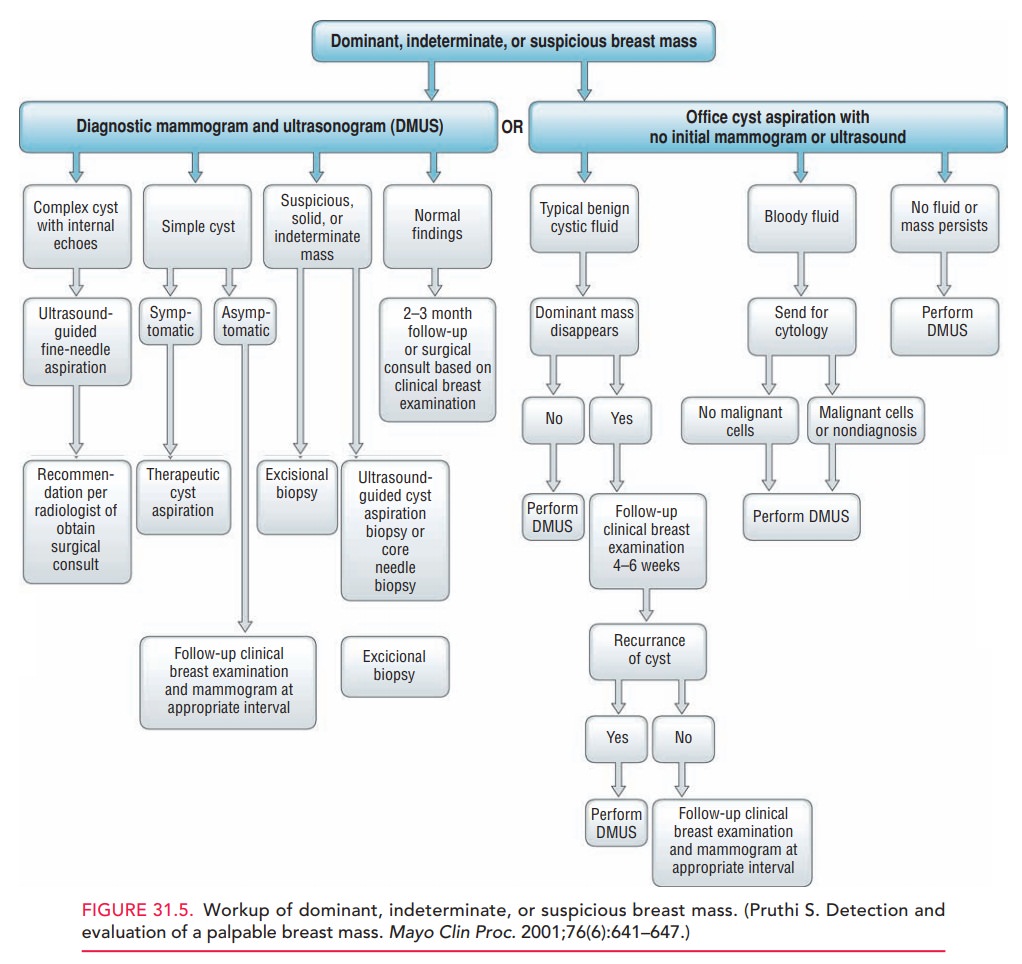
Diagnosis Algorithm
If a breast mass is found through a clinical breast exami-nation, self-examination, or historically by a patient, the clinician must clearly document the finding and assign appropriate follow-up care. Figure 31.5 presents a practi-cal algorithm for the evaluation and follow-up of a patient with a breast mass.
Related Topics