Chapter: Medical Surgical Nursing: Assessment of Digestive and Gastrointestinal Function
Endoscopic Procedures - Diagnostic Evaluation of Digestive and Gastrointestinal Function
ENDOSCOPIC
PROCEDURES
Endoscopic
procedures used in GI tract assessment include
fibroscopy/esophagogastroduodenoscopy, anoscopy, proctoscopy, sigmoidoscopy,
colonoscopy, small-bowel enteroscopy, and endos-copy through ostomy.
Upper Gastrointestinal Fibroscopy/ Esophagogastroduodenoscopy
Fiberscopes are flexible scopes equipped with fiberoptic lenses. Fibroscopy of the upper GI tract allows direct visualizationof the esophageal, gastric, and duodenal mucosa through a lighted endoscope (gastroscope) (Fig. 34-5).
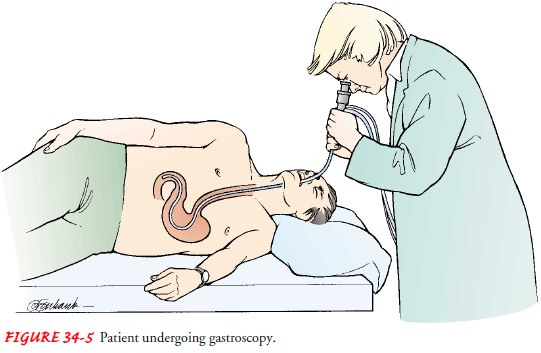
This procedure called
esophagogastroduodenoscopy (EGD), is especially valu-able when esophageal,
gastric, or duodenal abnormalities or in-flammatory, neoplastic, or infectious
processes are suspected. This procedure also can be used to evaluate esophageal
and gastric motility and to collect secretions and tissue specimens for further
analysis.
The
gastroenterologist views the GI tract through a viewing lens and can take still
or video photographs through the scope to document findings. Electronic video
endoscopes also are available that attach directly to a video processor,
converting the electronic signals into pictures on a television screen. This
allows larger and continuous viewing capabilities, as well as the simultaneous
record-ing of the procedure.
Side-viewing
flexible scopes are used to visualize the common bile duct and the pancreatic
and hepatic ducts through the am-pulla of Vater in the duodenum. This
procedure, called endo-scopic retrograde cholangiopancreatography (ERCP), uses
the endoscope in combination with radiographic techniques to view the ductal
structures of the biliary tract. ERCP is helpful in eval-uating jaundice,
pancreatitis, pancreatic tumors, common duct stones, and biliary tract disease.
Upper
GI fibroscopy also can be a therapeutic procedure when it is combined with
other procedures. Therapeutic endoscopy can be used to remove common bile duct
stones, dilate strictures, and treat gastric bleeding and esophageal varices.
Laser-compatible scopes can be used to provide laser therapy for upper GI
neo-plasms. Sclerosing solutions can be injected through the scope in an
attempt to control upper GI bleeding.
After
the patient is sedated, the endoscope is lubricated with a water-soluble
lubricant and passed smoothly and slowly along the back of the mouth and down
into the esophagus. The gastro-enterologist views the gastric wall and the
sphincters, and then advances the endoscope into the duodenum for further
examina-tion. Biopsy forceps to obtain tissue specimens or cytology brushes to
obtain cells for microscopic study can be passed through the scope. The
procedure usually takes about 30 minutes.
The
patient may experience nausea, gagging, or choking. Use of topical anesthetics
and moderate sedation makes it important to monitor and maintain the oral
airway during and after the procedure. Finger or ear oximeters are used to
monitor oxygen saturation, and supplemental oxygen may be used if needed.
Emergency equipment must be readily available. Precautions must be taken to
protect the scope, because the fiberoptic bundles can be broken if the scope is
bent at an acute angle. The patient wears a mouth guard to keep from biting the
scope.
NURSING INTERVENTIONS
The
patient should not eat or drink for 6 to 12 hours before the examination.
Patient preparation includes helping the patient spray or gargle with a local
anesthetic, and administering mida-zolam (Versed) intravenously just before the
scope is intro-duced. Midazolam is a sedative that provides moderate sedation
and relieves anxiety during the procedure. The nurse also may ad-minister
atropine to reduce secretions, and may give glucagon, if needed and prescribed,
to relax smooth muscle. The nurse posi-tions the patient on the left side to
facilitate saliva drainage and to provide easy access for the endoscope. After
the procedure, the nurse instructs the patient not to eat or drink until the gag
reflex returns (in 1 to 2 hours), to prevent aspiration of food or fluids into
the lungs. The nurse places the patient in the Simms posi-tion until he or she
is awake and then places the patient in the semi-Fowler’s position until ready
for discharge. After gastroscopy,assessment by the nurse includes observing for
signs of perfora-tion, such as pain, bleeding, unusual difficulty swallowing,
and an elevated temperature. The nurse monitors the pulse and blood pressure
for changes that can occur with sedation. The nurse can test the gag reflex by
placing a tongue blade onto the back of the throat to see whether gagging
occurs. After the patient’s gag re-flex has returned, the nurse can offer
lozenges, saline gargle, and oral analgesics to relieve minor throat
discomfort. Patients who were sedated for the procedure must stay on bed rest
until fully alert. After moderate sedation, the patient must be accompanied and
transported home if the procedure was performed on an out-patient basis. The
nurse instructs the patient not to drive for 10 to 12 hours if sedation was
used.
Anoscopy, Proctoscopy, and Sigmoidoscopy
The
lower portion of the colon also can be viewed directly to evaluate rectal
bleeding, acute or chronic diarrhea, or change in bowel patterns and to observe
for ulceration, fissures, abscesses, tumors, polyps, or other pathologic
processes. Rigid or flexible fiberoptic scopes can be used. The anoscope is a
rigid scope that is used to examine the anus and lower rectum. Proctoscopes and
sigmoidoscopes are rigid scopes that are used to inspect the rec-tum and the
sigmoid colon.
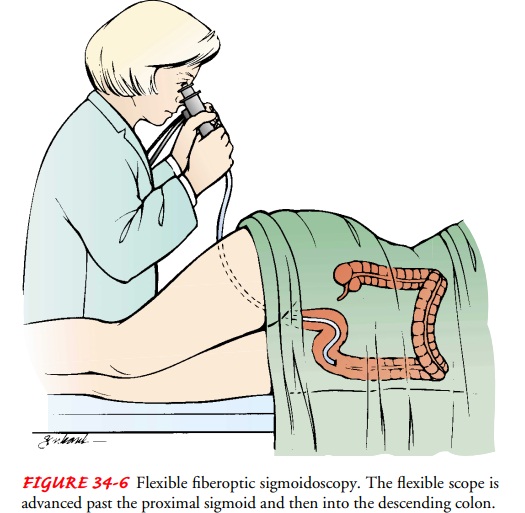
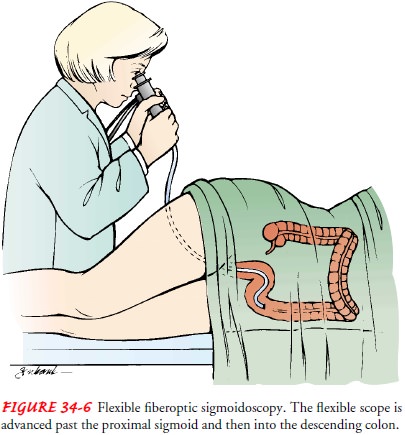
Flexible
scopes have largely replaced the rigid scopes for routine examinations. The
flexible fiberoptic sigmoidoscope (Fig. 34-6) permits the colon to be examined
up to 40 to 50 cm (16 to 20 inches) from the anus, much more than the 25 cm (10
inches) that can be visualized with the rigid sigmoidoscope. The flexible scope
has many of the same capabilities as the scopes used for the upper GI study,
including the use of still or video images to doc-ument findings.
For rigid scope procedures, the patient assumes the knee-chest position at the edge of the bed or the examining table. With the back inclined at about a 45-degree angle, the patient is properly positioned for the introduction of an anoscope, proctoscope, or sigmoidoscope. During the examination, it is important to keep the patient informed about the progress of the examination and to explain that the pressure exerted by the instrument will create the urge to have a bowel movement.
For
flexible scope procedures, the patient assumes a comfort-able position on the
left side with the right leg bent and placed anteriorly. Again, it is important
to keep the patient informed throughout the examination and to explain the
sensations asso-ciated with the examination. Biopsies and polypectomies can be
performed during this procedure. Biopsy is performed with small biting forceps
introduced through the endoscope; one or more small pieces of tissue may be
removed. If rectal or sigmoid polyps are present, they may be removed with a
wire snare, which is used to grasp the pedicle, or stalk. An electrocoagulating
cur-rent is then used to sever the polyp and prevent bleeding. It is extremely
important that all excised tissue be placed immedi-ately in moist gauze or in
an appropriate receptacle, labeled cor-rectly, and delivered without delay to
the pathology laboratory for examination.
NURSING INTERVENTIONS
These
examinations require only limited bowel preparation, in-cluding a warm tap
water or Fleet’s enema until returns are clear. Dietary restrictions usually
are not necessary, and sedation usu-ally is not required. During the procedure,
the nurse monitors vital signs, skin color and temperature, pain tolerance, and
vagal response (Society of Gastroenterologic Nursing and Associates, 2000).
After the procedure, the nurse monitors the patient for rectal bleeding and
signs of intestinal perforation (ie, fever, rectal drainage, abdominal
distention, and pain). On completion of the examination, the patient can resume
regular activities and dietary practices.
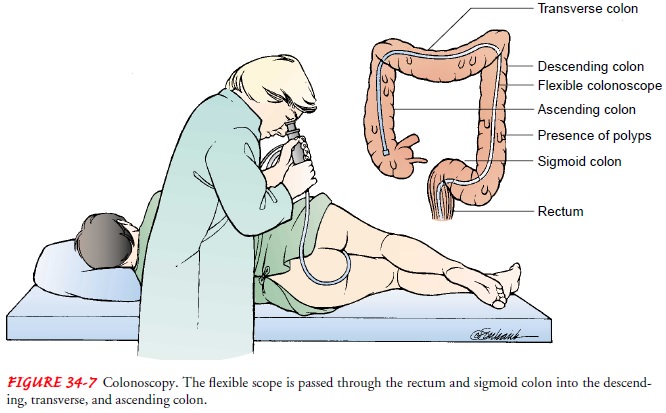
Fiberoptic Colonoscopy
Direct
visual inspection of the colon to the cecum is possible by means of a flexible
fiberoptic colonoscope (Fig. 34-7). These scopes have the same capabilities as
those used for esophagogastroduodenoscopy; however, they are larger in diameter
and longer. Still and video recordings can be used to document the procedure
and findings.
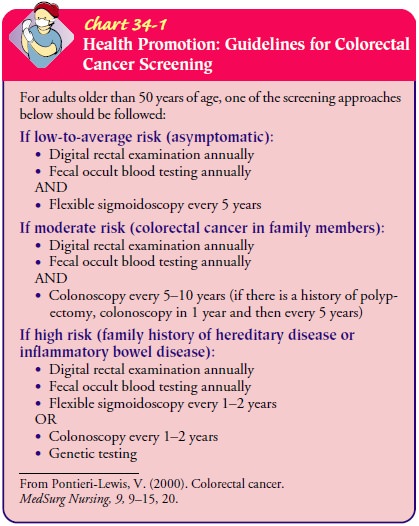
This
procedure is used commonly as a diagnostic aid and screening device. It is most
frequently used for cancer screening (see Chart 34-1) and for surveillance in
patients with previous colon cancer or polyps. In addition, tissue biopsies can
be obtained as needed, and polyps can be removed and evaluated. Other uses of
colonoscopy include the evaluation of patients with diarrhea of unknown cause,
occult bleeding, or anemia; further study of abnormalities detected on barium
enema; and diagnosis, clarifi-cation, and determination of the extent of
inflammatory or other bowel disease.
Therapeutically,
the procedure can be used to remove all vis-ible polyps with a special snare
and cautery through the colono-scope. Many colon cancers begin with adenomatous
polyps of the colon; therefore, one goal of colonoscopic polypectomy is early
detection and prevention of colorectal cancer. This procedure also can be used
to treat areas of bleeding or stricture. Use of bipolar and unipolar
coagulators, use of heater probes, and injections of sclerosing agents or
vasoconstrictors are all possible during this procedure. Laser-compatible
scopes provide laser therapy for bleed-ing lesions or colonic neoplasms. Bowel
decompression can also be completed during the procedure.
Colonoscopy is performed while the patient is lying on the left side with the legs drawn up toward the chest. The patient’s posi-tion may be changed during the test to facilitate advancement of the scope. The procedure usually takes about 1 hour. Discomfort may result from instillation of air to expand the colon or from insertion and moving of the scope. Biopsy forceps or a cytology brush may be passed through the scope to obtain specimens for histology and cytology examinations. Potential complications of colonoscopy include cardiac dysrhythmias and respiratory de-pression resulting from the medications administered, vasovagal reactions, and circulatory overload or hypotension resulting from overhydration or underhydration during bowel preparation. There-fore, it is important to monitor the patient’s cardiac and respiratory function continuously. Oxygen saturation is monitored with a finger or ear oximeter. Supplemental oxygen should be used as necessary.
NURSING INTERVENTIONS
The
success of the procedure depends on how well the colon is prepared. Adequate
colon cleansing provides optimal visualiza-tion and decreases the time needed
for the procedure. First, the patient should limit the intake of liquids for 24
to 72 hours be-fore the examination. Then, cleansing of the colon can be accom-plished
in various ways. The physician may prescribe a laxative for two nights before
the examination and a Fleet’s or saline enema until the return runs clear the
morning of the test. More frequently, however, polyethylene glycol electrolyte
lavage solu-tions (Golytely, Colyte, NuLytely) are used as intestinal lavages
for effective cleansing of the bowel. The patient maintains a clear liquid diet
starting at noon the day before the procedure. Then the patient ingests lavage
solutions orally at intervals over 3 to 4 hours. If necessary, the nurse can
give this solution through a feeding tube if the patient is unable to swallow.
Patients with a colostomy can receive this same bowel preparation. With the use
of lavage solutions, bowel cleansing is fast (rectal effluent is clear in about
4 hours) and is tolerated fairly well by most patients. Side effects of the
electrolyte solutions include nausea, bloating, cramps or abdominal fullness,
fluid and electrolyte imbalance, and hypothermia (patients are often told to
drink the preparation as cold as possible to make it more palatable). The side
effects are especially problematic for elderly patients, and sometimes they
have difficulty ingesting the required volume of solution. The use of lavage
solutions is contraindicated in patients with intestinal obstruction or
inflammatory bowel disease.
Additional
nursing actions include the following:
•
Instructing the patient not to take routine
medications when the lavage solution is ingested; the medications will not be
digested and therefore will be ineffective
•
Advising the diabetic patient to consult with his
or her physician about medication adjustment to prevent hyper-glycemia or
hypoglycemia resulting from dietary modifica-tions required in preparation for
the test
•
Instructing all patients, especially the elderly,
to maintain adequate fluid, electrolyte, and caloric intake while under-going
bowel cleansing
Special
precautions must be taken for some patients. Implant-able defibrillators and
pacemakers are at high risk for malfunction if electrosurgical procedures (ie,
polypectomy) are performed in conjunction with colonoscopy. A cardiologist
should be con-sulted before the test is performed, and the defibrillator should
be turned off. These patients require careful cardiac monitoring dur-ing the
procedure. Colonoscopy cannot be performed if there is a suspected or
documented colon perforation, acute severe diver-ticulitis, or fulminant
colitis. Therapeutic colonoscopy may be contraindicated in patients with
coagulopathies and in those re-ceiving anticoagulation therapy, because of the
high risk for excessive bleeding during and after the procedure. Nonsteroidal
anti-inflammatory agents (NSAIDs), aspirin, ticlopidine, and pen-toxifylline
must be discontinued before the test and for 2 weeks after the procedure.
Patients taking coumadin or heparin must consult the physician for specific
instructions. Those with pros-thetic heart valves or a history of endocarditis
require prophylactic antibiotics before the procedure.
Informed
consent is obtained before the test. The patient re-ceives nothing by mouth
(NPO) after midnight before the test,but most medications can be taken with a
small amount of water; the physician should be consulted about medication use.
Before the examination, the nurse may administer intravenously an opi-oid
analgesic or a sedative (eg, midazolam) to provide moderate sedation and
relieve anxiety during the procedure. Glucagon may be used, if needed, to relax
the colonic musculature and to reduce spasm during the test. Elderly or
debilitated patients may require a reduced dosage of these medications to
decrease the risks of oversedation and cardiopulmonary complications.
During
the procedure, the nurse monitors for changes in oxy-gen saturation, vital signs,
color and temperature of the skin, level of consciousness, abdominal
distention, vagal response, and pain intensity. After the procedure, patients
who were sedated are maintained on bed rest until fully alert. Some will have
abdomi-nal cramps caused by increased peristalsis stimulated by the air
in-sufflated into the bowel during the procedure. Immediately after the test,
the nurse observes the patient for signs and symptoms of bowel perforation (eg,
rectal bleeding, abdominal pain or disten-tion, fever, focal peritoneal signs).
If midazolam was used, the nurse explains its amnesic effects. It is important
to provide writ-ten instructions, because the patient may be unable to recall
ver-bal information. If the procedure is performed on an outpatient basis,
someone must accompany and transport the patient home. After a therapeutic
procedure, the nurse instructs the patient to report any bleeding to the
physician.
Small-Bowel Enteroscopy
Technology
for the use of the small-caliber transnasal endoscope to allow direct
inspection of the wall of the small intestine continues to be developed. Two
methods are being used at this time: the “push” and the “pull” endoscope
methods. The “pull” endoscope is very long and flexible and has a balloon at
its tip. When inflated, the balloon tip advances the scope by peristalsis
through the small intestine. Reglan may be administered intravenously to assist
pas-sage. This procedure takes up to 10 hours to complete. The pa-tient may be
kept in the recovery area or sent home during this period. Once the scope has
entered the distal ileum, the balloon is deflated and the tube is retracted
slowly while the endoscopist examines the intestinal wall. “Push” endoscopes
have been designed to be smaller in caliber and longer in length, while still
allowing the use of biopsy forceps and probes (Lightdale, 2000). These two
methods are especially useful in the evaluation of patients who have continued
bleeding even after extensive diagnostic testing has identified no other
problem area. They can also be used when biopsy of the small bowel is needed to
diagnose malabsorption syndromes.
Endoscopy Through Ostomy
Endoscopy
using a flexible endoscope through an ostomy stoma is useful for visualizing a
segment of the small or large intestine. It may be indicated to evaluate an
anastomosis, to screen for re-current disease, or to visualize and treat
bleeding in a segment of the bowel. Nursing interventions are similar to those
for other endoscopic procedures.
Related Topics