Chapter: Clinical Anesthesiology: Anesthetic Management: Hepatic Physiology & Anesthesia
Effect of Anesthesia on Hepatic Function
EFFECT OF ANESTHESIA ON HEPATIC FUNCTION
Hepatic blood flow usually decreases during
regional and general anesthesia, and multiple factors are responsible,
including both direct and indirect effects of anesthetic agents, the type of
ventilation employed, and the type of surgery being performed.
Decreases in cardiac output reduce hepatic blood flow via reflex
sympathetic activation, which vasoconstricts both the arterial and the venous
splanchnic vasculature.
The hemodynamic effects of ventilation can
also have a significant impact on hepatic blood flow. Controlled
positive-pressure ventilation with high mean airway pressures reduces venous
return to the heart and decreases cardiac output; both mecha-nisms can compromise hepatic blood flow. The former increases
hepatic venous pressure, whereas the latter can reduce blood pressure and
increase sympathetic tone. Positive end-expiratory pressure (PEEP) further
accentuates these effects.
Surgical procedures near the liver can reduce hepatic blood flow up to
60%. Although the mecha-nisms are not clear, they most likely involve
sympa-thetic activation, local reflexes, and direct compression of vessels in
the portal and hepatic circulations.
β-Adrenergic blockers, α1-adrenergic ago-nists, H2-receptor
blockers, and vasopressin reduce hepatic blood flow. Low-dose dopamine
infusions may increase liver blood flow.
Metabolic Functions
The effects of the various anesthetic agents
on inter-mediary hepatic metabolism involving carbohy-drate, fat, and protein
are poorly defined. An endocrine stress response secondary to fasting
andsurgical trauma is generally observed. The neuroendocrine stress response to
surgery andtrauma is characterized by elevated circulating levels of
catecholamines, glucagon, and cortisol and results in the mobilization of
carbohydrate stores and pro-tein, causing hyperglycemia and negative nitrogen
balance (catabolism). The neuroendocrine stress response may be at least partially
blunted by regional anesthesia, deep general anesthesia and/or pharma-cological
blockade of the sympathetic system, with regional anesthesia having the most
salutary effecton catabolism. All opioids can potentially cause spasm of the
sphincter of Oddi andincrease biliary pressure. Naloxone
and glucagon may relieve opioid-induced spasm.
Procedures in close proximity to the liver
frequently result in modest elevations in lactate dehy-drogenase and
transaminase concentrations regard-less of the anesthetic agent or technique
employed.When the results of liver function tests are ele-vated
postoperatively, the usual cause is under-lying liver disease or the surgical
procedure itself. Persistent abnormalities in liver tests may be indica-tive of
viral hepatitis (usually transfusion related), sepsis, idiosyncratic drug
reactions, or surgical com-plications. Postoperative jaundice can result from a
variety of factors (Table 32–6), but the most com-mon cause is overproduction
of bilirubin because of resorption of a large hematoma or red cell breakdown
following transfusion. Nonetheless, all
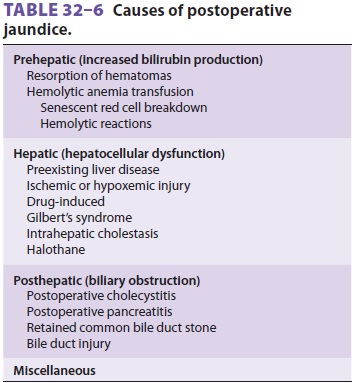
other causes should be considered. Correct
diagnosis requires a careful review of preoperative liver func-tion and of
intraoperative and postoperative events, such as transfusions, sustained
hypotension or hypoxemia, and drug exposure. Currently utilized volatile
anesthetic agents have minimal, if any, direct adverse effect upon hepatocytes.
Related Topics