Chapter: Medical Surgical Nursing: Assessment and Management of Problems Related to Male Reproductive Processes
Disorders of Male Sexual Function
Disorders of Male Sexual Function
ERECTILE DYSFUNCTION
Erectile dysfunction, also called impotence, is the inability
toachieve or maintain an erection sufficient to accomplish inter-course. The
man may report decreased frequency of erections, inability to achieve a firm
erection, or rapid detumescence (sub-siding of erection). Incidence ranges from
25% to 50% in men older than 65 years of age. The physiology of erection and
ejacu-lation is complex and involves sympathetic and parasympathetic
components. At the time of erection, pelvic nerves carry parasym-pathetic
impulses that dilate the smaller blood vessels of the re-gion and increase
blood flow to the penis, expanding the corpora cavernosa
Erectile
dysfunction has both psychogenic and organic causes. Psychogenic causes include
anxiety, fatigue, depression, and pressure to perform sexually. Organic
impotence, however, may account for more impotence than previously realized.
Organic causes include occlusive vascular disease, endocrine disease (diabetes,
pituitary tumors, hypogonadism with testosterone deficiency, hyperthyroidism,
and hypothyroidism), cirrhosis, chronic renal failure, genitouri-nary
conditions (radical pelvic surgery), hematologic conditions (Hodgkin’s disease,
leukemia), neurologic disorders (neuropathies, parkinsonism, spinal cord
injury, multiple sclerosis), trauma to the pelvic or genital area, alcohol,
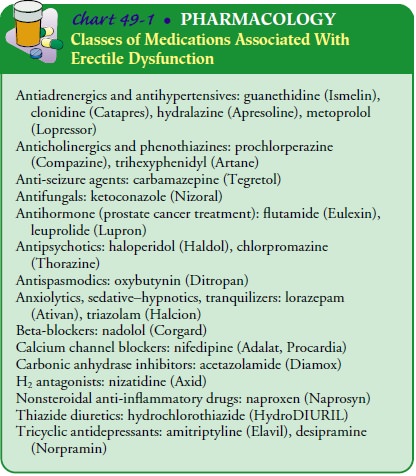
medications (Chart 49-1), and drug abuse.
Assessment and Diagnostic Findings
The diagnosis of erectile dysfunction requires a sexual and medical history; an analysis of presenting symptoms; a physical examination, including a neurologic examination; a detailed assessment of all medications, alcohol, and drugs used; and various laboratory studies. Nocturnal penile tumescence tests are conducted in sleep laboratories to monitor changes in penile circumference. In healthy men, nocturnal penile erections closely parallel rapid eye movement (REM) sleep in occurrence and duration. Organically impotent men show inadequate sleeprelated erections that correspond to their waking performance. The nocturnal penile tumescence test can help to determine whether erectile impotence has an organic or psychological cause. Arterial blood flow to the penis is measured using a Doppler probe. In addition, nerve conduction tests and extensive psychological evaluations are carried out. Figure 49-3 describes the evaluation and treatment of men with erectile dysfunction.
Medical Management
Treatment, which depends on the cause, can be
medical, surgi-cal, or both (Table 49-2). Nonsurgical therapy includes treating
associated conditions, such as alcoholism, and readjusting hyper-tensive agents
or other medications. Endocrine therapy may be instituted for erectile
dysfunction secondary to hypothalamic-pituitary-gonadal dysfunction and may
reverse the condition. In-sufficient penile blood flow may be treated with
vascular surgery. Patients with erectile dysfunction from psychogenic causes
are re-ferred to a health care provider or therapist specializing in sexual
dysfunction. Patients with erectile dysfunction secondary to or-ganic causes
may be candidates for penile implants.
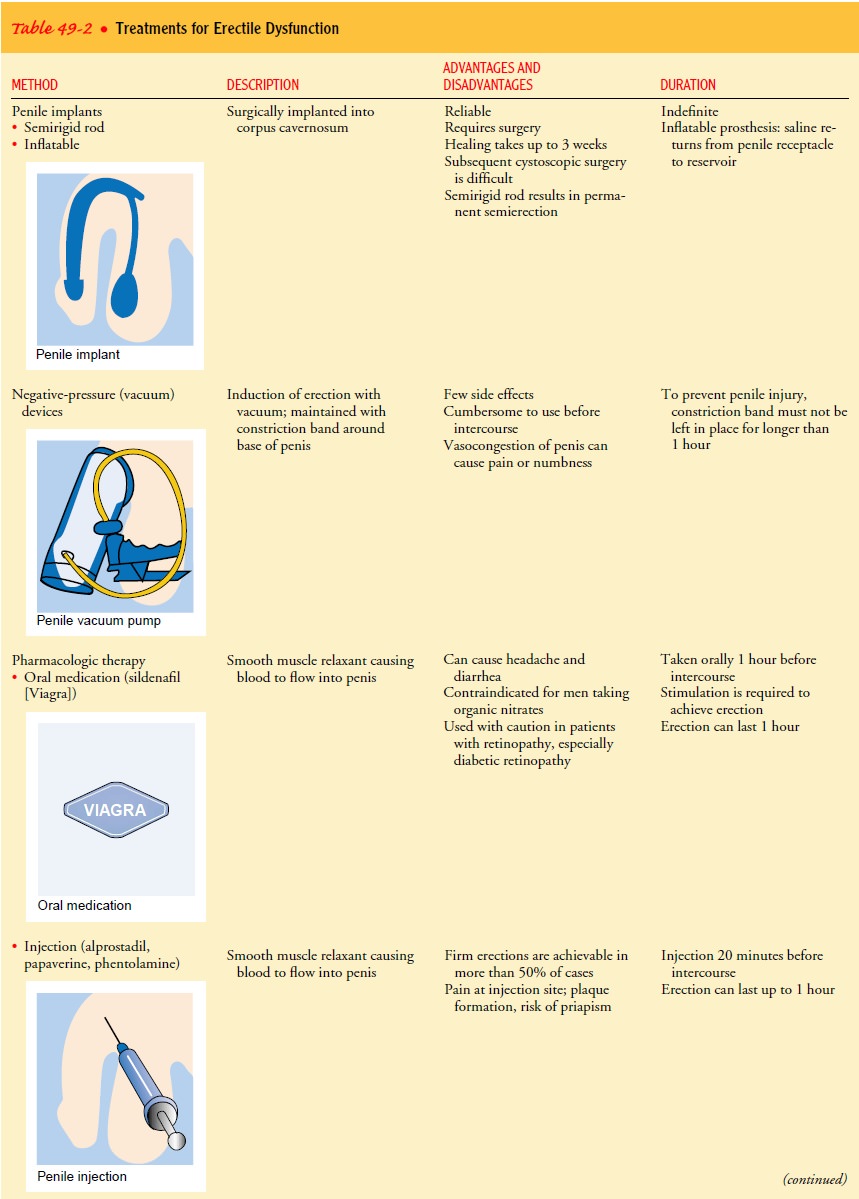
PHARMACOLOGIC THERAPY
Sildenafil (Viagra) is an oral medication for
erectile dysfunction (Eid, 2000). When it is taken about 1 hour before sex, an
erec-tion can occur with stimulation; the erection can last about 60 to 120
minutes. Despite the effectiveness of this medication, it does have side
effects: headache, flushing, and dyspepsia. Sildenafil is contraindicated in
patients who take organic nitrates and should be used with caution in patients
with retinopathy, especially those with diabetic retinopathy (Chart 49-2).
Other pharmacologic measures to induce
erections include in-jecting vasoactive agents, such as alprostadil,
papaverine, and phen-tolamine, directly into the penis. Complications include priapism (a persistent abnormal
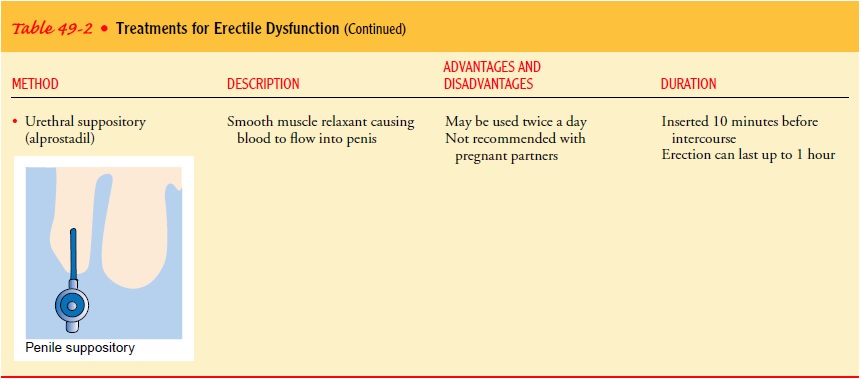
erection) and development of fibrotic plaques at the injection sites. Alprostadil
is also formulated in a gel pellet that can be inserted into the urethra to
create an erection.
PENILE IMPLANTS
Penile implants are available in two types:
the semirigid rod and the inflatable prosthesis. The semirigid rod (eg, the
Small-Carrion prosthesis) leaves the man with a permanent semierection. The
inflatable prosthesis simulates natural erections and natural flac-cidity.
Complications after implantation include infection, erosion of the prosthesis
through the skin (more common with the semi-rigid rod than with the inflatable
prosthesis), and persistent pain, which may require removal of the implant.
Cystoscopic surgery, such as transurethral
resection of the prostate (TUR or TURP), is more difficult with a semirigid
rod than with the inflatable prosthesis. Factors to consider in choosing a
prosthesis are the pa-tient’s activities of daily living and social activities
and the expec-tations of the patient and his partner. Ongoing counseling for
the patient and his partner is usually necessary to help them in adapt-ing to
the prosthesis.
NEGATIVE-PRESSURE DEVICES
Negative-pressure
(vacuum) devices may also be used to induce an erection. A plastic cylinder is
placed over the flaccid penis, and negative pressure is applied. When an
erection is attained, a con-striction band is placed around the base of the
penis to maintain the erection. Although many men find this method
satisfactory, others experience premature loss of penile rigidity or pain when
applying suction or during intercourse.
Nursing Management
Personal satisfaction and the ability to
sexually satisfy a partner are common concerns of patients. Men with illnesses
and disabilities may need the assistance of a sex therapist to find, implement,
and integrate their sexual beliefs and behaviors into a healthy and satisfying lifestyle. The
nurse can inform patients that support groups for men with erectile dysfunction
and their partners have been es-tablished.
EJACULATION PROBLEMS
Premature ejaculation occurs when a man
cannot control the ejac-ulatory reflex and, once aroused, reaches orgasm before
or shortly after intromission. It is the most common dysfunction in men.
In-hibited or retarded ejaculation is the involuntary inhibition of the
ejaculatory reflex. The spectrum of responses includes occasional ejaculation
through intercourse or self-stimulation or the com-plete inability to ejaculate
under any circumstances.
Treatment modalities depend on the nature and
severity of the ejaculation problem. Behavioral therapies may be indicated for
people with premature ejaculation; these therapies often involve the man and
his sexual partner. “Homework” assignments are often given to the couple to
encourage them to identify their sexual needs and to communicate those needs to
each other. In some cases, pharmacologic and behavioral therapy together may be
effective.
Neurologic disorders (eg, spinal cord injury,
multiple sclero-sis, neuropathy secondary to diabetes), surgery
(prostatectomy), and medications are the most common causes of inhibited ejac-ulation.
Chemical, vibratory, and electrical stimulation have been used with some
success. Treatment is usually multidisciplinary and addresses the physical and
psychological factors that are often involved in inhibited ejaculation (Lue,
2000).
For men with retrograde ejaculation, the
urine may be col-lected after ejaculation; sperm is then collected from the
urine for use in artificial insemination. In men with spinal cord injury,
electroejaculation may be used to obtain sperm for artificial in-semination.
The effects of trauma, chronic illness, and
physical disability on sexual function can be profound. In addition to
psychogenic factors, the physical changes associated with illness and injury
can impair sexual function.
Related Topics