Chapter: 11th 12th std standard Class Nursing Health Care Hospital Hygiene Higher secondary school College Notes
Cleft lip and cleft palate - Parental advice and Treatment
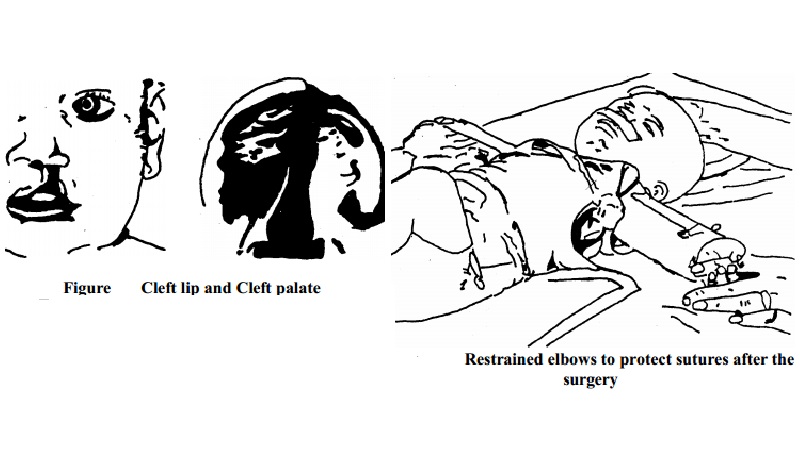
Cleft
lip and cleft palate:
Cleft lip and cleft palate results
when fusion involving a first brachial arch fails to take shape during
embryonic development.
1. The cleft lip: It results from the failure of maxillary
processes to fuse with the nose elevation on the frontal prominence. This
defect varies from a notch in the lip to complete separation of the lip into a
hare. The cleft lip may be unilateral or bilateral.
2. Cleft palate (isolated): Isolated cleft palate results from
a failure of the fusion of secondary palate with each other, and with the
primary palate. It can be unilateral or bilateral.
3. Cleft lip and palate: This condition results from a combined
defect of cleft lip and cleft palate.
4. Administration of the drugs: The parents should be explained
about the side effects of the drugs used over a long period and about the
regular use of the drugs.
5.
Any side effect such as neuritis,
jaundice, rash, hearing disorder, and renal problem should be reported,
promptly, to the doctor. The parents should be helped to relieve the anxiety
and to avoid overprotection.
Parental advice:
The parents should be instructed to continue the treatment
until the disease is cured and until the doctor orders to discontinue.
1.
The parents and, if applicable,
children should be instructed about the proper coughing and sneezing technique
by covering the mouth and nose to prevent droplet infection.
2.
The parents should be explained
about the use of B.C.G. vaccination for other young children if necessary.
3.
The importance of nutritious diet
should be emphasized, to develop the resistance in the children.
Preventive Measures:
1. Early detection of condition and prompt treatment can help
to prevent complications.
2.
Case finding and follow-up of known
contact can help to control the infection.
3.
Periodic skin testing of children
for tuberculosis.
4.
Prophylactic anti-tuberculosis drugs
may be prescribed to those who have high risk of tuberculosis.
5.
Improving living conditions, if
possible, is advisable.
Investigations:
Cleft lip with or without the cleft palate is easily
apparent at birth. Only cleft palate may be identified when thorough assessment
of the mouth is done or when the infant has difficulty with initial feeding.
Treatment:
Treatment of cleft lip and cleft
palate may require joint efforts of pediatrician, plastic surgeon, nurses,
orthodontist, prosthodontist, and speech therapist.
Surgical Treatment:
1.
Closure of the cleft lip is done
first .and then the closure of the cleft palate is done. The time for the
surgery of the lip varies. Some prefer the lip closure immediately after birth
whereas others may prefer to wait for two to-three months until the child gains
adequate weight.
2. The cleft lip is generally repaired by Z-shaped sutures, to
reduce notching of the lip. After the surgery, the suture line is protected
from tension by an arched metal device taped to the cheek.
3.
Cleft palate surgery is postponed
later in order to wait for the changes in the palate. Many surgeons prefer to
do it between the age one and two years, before the child develops defective
speech.
4.
Orthodeontic and prosthodontic
treatment may be required to correct malposition of the teeth and maxillary
arch. Children with cleft palate may have speech problem and may require speech
therapy.
Management:
1. Soon after the birth, the baby may look unattractive but the
nurse should not show her reactions.
2.
The disfiguring defect may cause negative
reaction and shock in the parents.
3.
The nurse should explain the
positive aspects about the correction of the defect and other possible
treatment.
4.
Feeding of an infant: The immediate
problem faced is the feeding an infant with the cleft lip and palate, because
this defect reduces the ability of the infant to suck.
5.
While feeding, the infant should be
held in upright position. A special cleft palate nipple can be used. A large
and soft nipples with the large hole or a long and soft lamb's nipples are
useful.
6.
When the infants have the problem to
take feeds with the nipple, a syringe with the rubber tube may be used to feed.
Pre-operative care:
1.
The mother should be explained about
the proper breast-feeding and that of the bottle-feeding, to help the infant
gain weight.
2.
The infants should be encouraged to.
lie on its back to practise for postoperative essential positioning, especially
with the arm restraints.
3.
Parents should be motivated to
provide love and affection to develop an attachment.
Instructions should be given to give the last feed six hours
before the surgery.
Post-operative care:
Assessment of the vital signs should be done and the general
post operative care should be provided. Side lying position helps to drain the
secretions and prevent aspiration.
Protection of the surgical sutures at the site of the repair
is done by the followings:
The patient is positioned on the back or side for the
repaired cleft lip. Positioning on the abdomen is useful for the palate
surgery.
Maintaining the protective device on the sutures.
Restraining the arms by elbow restraints helps to protect the infants' hands
reaching the suture line.
1.
The infection can be prevented by
the cleaning the operated area, gently, with the aseptic precautions after each
feeding and avoiding contamination.
2.
An injury should be prevented by
prevention of any object putting in the mouth.
3.
Love, affection and security can be
provided by cuddling of the infant.
4.
Parental support may be required to
clear their doubts and encourage them to accept the baby.
Parental advice:
1.
Explain the routine care of the
baby.
2.
Demonstrate the technique of
feeding.
3.
Refer to the genetic counseling
clinic.
4.
Refer to social agencies and other
agencies.
5.
Explain about the follow-up.
Related Topics