Chapter: Medicine and surgery: Gastrointestinal system
Cholera - Gastrointestinal infections
Cholera
Definition
Cholera is an acute infection of the gastrointestinal tract caused by the Gramnegative bacterium Vibrio cholera.
Incidence
66 cases in the past 20 years in the United Kingdom, endemic in South East Asia and South America.
Aetiology
V. cholera is found free living in fresh water, it is only pathogenic in humans. It can contaminate shellfish. Transfer from human carriers is via the faeco–oral route.
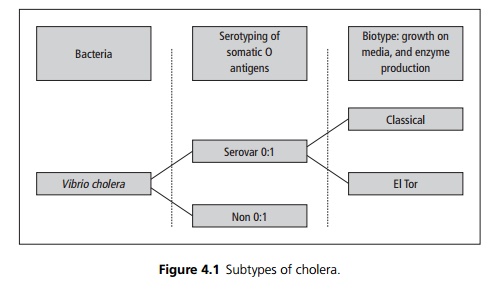
The serovar 0:1 is the major pathogenic strain and is divided into two biotypes; classical and the more widespread El Tor (named after the quarantine camp in which it was discovered). Phage typing can be used to examine epidemics to try and see if the observed conditions originated from a single source (see Fig. 4.1).
Pathophysiology
1. V. cholera is damaged by stomach acid therefore patients on acid suppressing medication are particularly susceptible to infection.
2. Once in the small bowel proliferation occurs and there is production of an exotoxin.
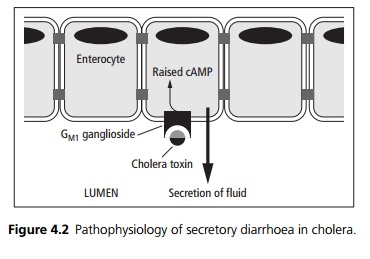
3. The B subunit of the exotoxin binds to intestinal epithelium expressing the GM1 ganglioside and the A unit activates adenylate cyclase (see Fig. 4.2). The result is an increase in cellular levels of cAMP and massive secretion of isotonic fluid into the intestinal lumen.
4. A second toxin termed zonula occludens toxin (ZOT) damages the tight junctions between enterocytes allowing the passage of water and electrolytes.
Clinical features
The incubation period is between a few hours and 1 week. Most patients have a mild selflimiting diarrhoeal illness but in severe cases there may be watery diarrhoea with mucous, termed rice water stool. It is vital to adequately fluid resuscitate patients with such diarrhoea to prevent the onset of hypovolaemic shock.
Investigations
The diagnosis is often made on clinical features alone, pending the results of stool cultures which are diagnostic. However, stool microscopy may reveal the characteristic motile organisms.
Management
This depends on disease severity. Assessment of hypovolaemia may be made using clinical indices such as the difference between lying and standing blood pressure, the heart rate, skin turgor, urine output and urea and electrolyte measurement. A postural drop of 15 mmHg or more suggests volume depletion.
· In significant volume depletion intravenous saline should be administered. The fluid input and output should be documented hourly and reviewed with care.
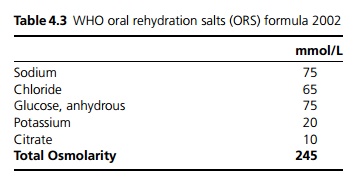
· In mild cases oral rehydration is the treatment of choice using a solution containing sodium, potassium, chloride and citrate. Traditional solutions use glucose to facilitate absorption, ricebased polymers have been used in place of glucose with some evidence of benefit in reducing duration of diarrhoea (see Table 4.3).
· Tetracycline or ciprofloxacin can be used to shorten duration and reduce severity of illness.
Related Topics