Chapter: Essentials of Psychiatry: Anxiety Disorders: Panic Disorder With and Without Agoraphobia
Anxiety Disorders: Panic Disorder With and Without Agoraphobia
Anxiety Disorders: Panic Disorder With and Without
Agoraphobia
Definitions and Diagnostic Criteria
According to the Diagnostic and
Statistical Manual of Mental Disorders,
Fourth Edition, Text Revision (DSM-IV-TR) (Ameri-can Psychiatric Association,
2000), panic disorder is defined by recurrent and unexpected panic attacks. At
least one of these at-tacks must be followed by one month or more of:
·
persistent concern about having more attacks;
·
worry about the implications or consequences of the
attack; or
·
changes to typical behavioral patterns (e.g.,
avoidance of work or school activities) as a result of the attack
In addition, the panic attacks must not stem solely from the direct
effects of illicit substance use, medication, or a general medical condition
(e.g., hyperthyroidism, vestibular dysfunction) and are not better explained by
another mental disorder (e.g., such as social phobia for attacks that occur
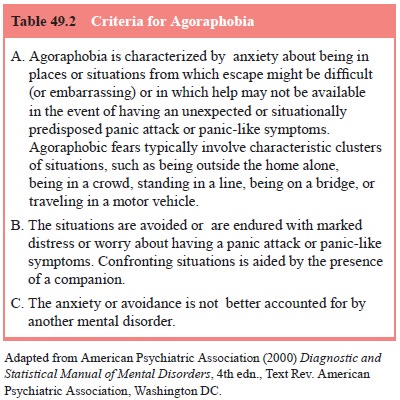
only in social situations). A diagnosis of panic disorder with agoraphobia is
warranted when the criteria for panic disorder are satisfied and accompanied by
agoraphobia.
Although panic attacks are a cardinal feature of panic dis-order and in
combination with agoraphobia (i.e., anxiety about be-ing in a place or a situation
that is not easily escaped or where help is not easily accessible if panic
occurs) are essential to a diagno-sis of panic disorder with agoraphobia, the
criteria sets for panic attacks and for agoraphobia are listed separately as
standalone noncodable conditions that are referred to by the diagnostic
cri-teria for panic disorder and agoraphobia without history of panic disorder.
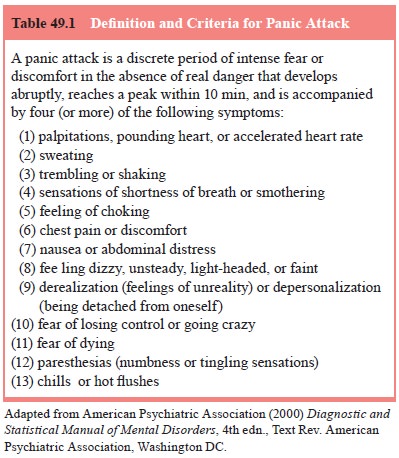
Notwithstanding, accurate diagnosis is difficult without a proficient
understanding of these features. Tables 49.1 and 49.2 show the DSM-IV-TR
criteria for panic attack and agoraphobia, respectively. While the criteria for
agoraphobia are generally straightforward, panic attacks can be difficult to
understand.
A number
of investigations indicate that people report hav-ing what they consider to be
a panic attack during or in association with actual physical threat (i.e., a
true alarm situation). It is, how-ever, important to distinguish between a fear
reaction in response to actual threat and a panic attack. In an attempt to do so,
the DSM-IV-TR has clarified that panic attacks occur “in the absence of real
danger”. Such attacks involve a paroxysmal occurrence of intense fear or
discomfort accompanied by a minimum of four of the 13 symptoms shown in Table
49.1. The DSM-IV-TR recognizes three characteristic types of panic attacks,
including those that are unex-pected (i.e., not associated with an identifiable internal
or external trigger and appear to occur “out of the blue”), situationally bound
(i.e.,
almost invariably occur when exposed to a situational trigger or when
anticipating it) and situationally predisposed (i.e., usually, but not
necessarily, occur when exposed to a situational trigger or when anticipating
it). The term limited symptom attacks is used to refer to panic-like
episodes comprising fewer than four symptoms.
Although unexpected panic attacks are required for a diag-nosis of panic
disorder, not all panic attacks that occur in panic dis-order are unexpected.
The occurrence of unexpected attacks can wax and wane and over the
developmental course of the disorder they tend to become situationally bound or
predisposed. Moreo-ver, unexpected panic attacks as well as those that are
situationally bound or predisposed can occur in the context of other psychiatric
disorders, including all of the other anxiety disorders, e.g., a per-son with
social phobia might have an occasional unexpected panic attack without the
other feature required to diagnose panic disor-der; a dog phobic might panic
whenever a large dog is encountered) and some general meda conditions. A clear
understanding of the
distinction between types of panic attacks outlined in the DSM-IV-TR
provides a foundation for diagnosis and differential diag-nosis. However,
consideration of other characteristics of panic – including duration of
attacks, frequency of attacks, number and intensity of symptoms, nature of
catastrophic thinking and mech-anism responsible for termination of an attack –
can be important in identifying exacerbating and controlling factors.
Related Topics