Chapter: Essential Anesthesia From Science to Practice : Clinical management : Pre operative evaluation
Anesthetic choice - Anesthesia Clinical management
Anesthetic choice
In
addition to the above assessment, the anesthetic plan must consider the wishes
of both patient and surgeon, as well as our
individual skill and experience. Does the patient have special requests that
need to be taken into account? For example, some patients would like to be
awake (maybe the President so he doesn’t have to pass control of the US to the
Vice-President), others asleep, and others do not want “a needle in the back.”
Some
patients present special problems, for example Jehovah’s Witnesses who do not
accept blood transfusions, based on their interpretation of several pas-sages
in the Bible (for example Acts 15:28, 29). A thoughtful and compassion-ate
discussion with the patient usually finds the physician agreeing to honor the
patient’s wishes, an agreement that may not be violated. The caring for
children of Jehovah’s Witnesses brings an added concern and may require ethics
consultation and perhaps even referral to a court. Again, these issues are best
brought out days prior to surgery at a scheduled pre-anesthetic evaluation.
Numerous
studies have failed to demonstrate that a particular inhalation anes-thetic,
muscle relaxant, or narcotic made for a better outcome than an alternative.
Yet, over the years, actual or perceived differences and conveniences have
caused some drugs to disappear and others to establish themselves. Given an array
of options, we can often consider different approaches to anesthesia, which we
can discuss with the patient. We should always recommend the approach with
which we have the greatest experience and which we would select for ourselves
or a loved one.
The choices
depend on several factors, first of which is the surgical procedure. For
example, the site of the operation, e.g., a craniotomy, can rule out spinal
anesthesia. The nature of the operation, e.g., a thoracotomy, can compel us to
use an endotracheal tube. For the removal of a wart or toenail or the lancing
of a boil, we would not consider general anesthesia – unless the patient’s age
or psychological condition would make it preferable. The preferences of the
surgeon might also be considered.
This
introduces the patient’s condition as a factor in the choice of anesthesia. For
example, a patient in hemorrhagic shock depends on a functioning sym-pathetic
nervous system for survival and therefore cannot tolerate the sympa-thetic
blockade induced by spinal or epidural anesthesia. A patient with an open eye
can lose vitreous if the intra-ocular pressure rises, as might occur with the
use of succinylcholine. Vigorous coughing at the end of an eye operation might
do the same and must be avoided. Respiratory depression and elevated arterial
carbon dioxide levels can increase intracranial pressure with potentially
devas-tating effects in patients with an intracranial mass or hemorrhage. In
obstetri-cal anesthesia, mother and
child have to be considered. Here, we do not wish to depress uterine
contraction nor cause prolonged sedation of the newborn child. Some agents used
in anesthesia rely on renal excretion, others on hepatic metabolism, thus
tilting our choice of drugs in patients with renal or hepatic insufficiency.
In the
majority of patients, however, it makes little difference what we pick. We
could choose one or the other technique for general anesthesia, using one or
the other intravenous induction drug and neuromuscular blocker, and relying on
one or the other inhalation anesthetic. We can supplement such a technique with
one of a number of narcotic drugs available to us, or we can use total
intravenous anesthesia. When we use general anesthesia, we can intubate the
patient’s trachea and let the patient breathe spontaneously, or we can
artificially ventilate the patient’s lungs. Instead of an endotracheal tube, we
have available the laryngeal mask airway, preferably used in spontaneously
breathing patients or, in the very old-fashioned approach, we might use only a
face mask.
In many
instances, we have options, the choice of which will be influenced by our own
experience and expertise. For example, anesthesiologists with extensive
experience in regional anesthesia will select that technique in preference to
gen-eral anesthesia in cases where either technique can prove satisfactory for
patient and surgeon. Examples include many orthopedic operations or procedures
on the genitourinary tract.
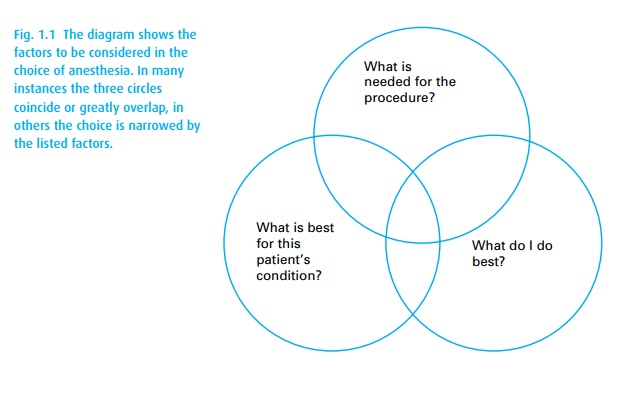
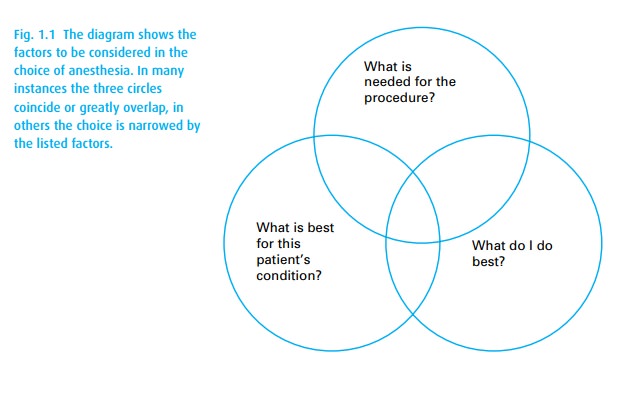
In
summary, many factors can influence the choice of anesthesia. In the major-ity
of patients, however, we have the luxury of making the choice influenced by our
own preference and routine (Fig. 1.1).
Related Topics