Chapter: Obstetrics and Gynecology: Hirsutism and Virilization
Androgen Production and Androgen Action
ANDROGEN PRODUCTION AND ANDROGEN ACTION
In women, androgens are produced in the adrenal glands, the ovaries, and
adipose tissue, where there is extraglan-dular production of testosterone from
androstenedione. The following three androgens may be measured when evaluating
a woman with hirsutism and virilization.
·
Dehydroepiandrosterone
(DHEA): a weak androgensecreted principally by the
adrenal glands. (This is gen-erally measured as dehydroepiandrosterone sulfate
[DHEA-S] because of its longer half-life, making it a more reliable measure.)
·
Androstenedione:
a weak androgen secreted in equalamounts by the
adrenal glands and ovaries.
·
Testosterone:
a potent androgen secreted by theadrenal glands and
ovaries and produced in adipose tis-sue from the conversion of androstenedione.
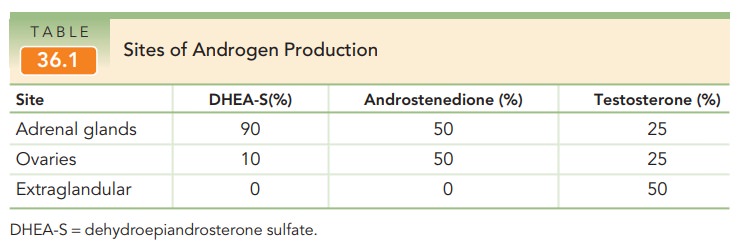
The sites of androgen production
and proportions pro-duced are presented in Table 36.1. In addition,
testosterone is also converted within hair follicles and within genital skin to
dihydrotestosterone (DHT), which is
an androgen even more potent than testosterone. This metabolic con-version is
the result of the local action of 5α-reductase on testosterone at these sites. This is
the basis for constitu-tional hirsutism, which is discussed later.
Adrenal androgen production is
controlled by recip-rocal feedback regulation through pituitary secretion of
adrenocorticotropic hormone (ACTH). ACTH stimulates the adrenal cortical
production of cortisol. In the metabolic
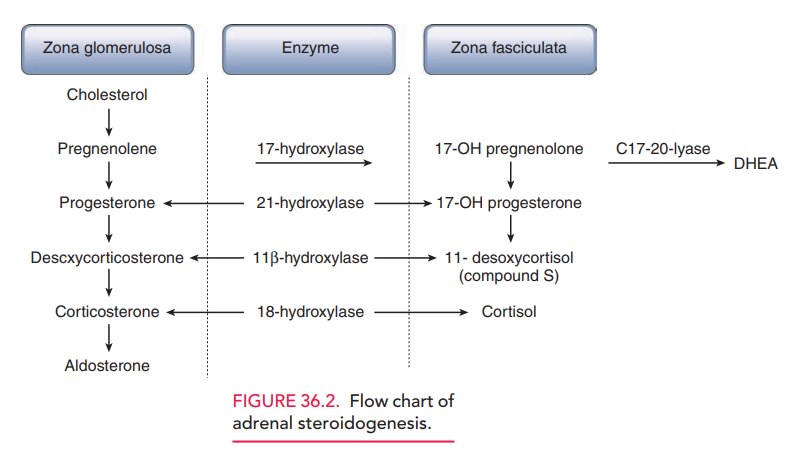
In enzymatic deficiencies of adrenal
steroidoge-nesis (21-hydroxylase deficiency and 11β-hydroxylase defi-ciency), DHEA
accumulates and is further metabolized to androstenedione and testosterone. The
flow of adrenal hormone production is shown in Figure 36.2.
Ovarian androgen production is
regulated by luteiniz-ing hormone (LH) secretion from the pituitary gland. LH
stimulates theca-lutein cells surrounding the ovarian fol-licles to secrete
androstenedione and, to a lesser extent, testosterone. These androgens are
precursors for estrogen production by granulosa cells of the ovarian follicles.
In conditions of sustained or increased LH secretion, andro-stenedione and
testosterone increase.
Extraglandular testosterone
production occurs in adi-pocytes (fat cells) and depends on the magnitude of
adrenal and ovarian androstenedione production. When andro-stenedione
production increases, there is a dependent increase in extraglandular
testosterone production. When a woman becomes obese, the conversion of
androstene-dione to testosterone is increased.
Testosterone is the primary androgen that causes increased hair growth, acne, and the physical changes associated with viril-ization. After testosterone is secreted, it is bound to a carrierprotein—sex hormone-binding globulin (SHBG)—and primarily circulates in plasma as a bound steroid hormone. Bound testosterone is unable to attach to testosterone receptors and is, therefore, metabolically inactive. Only a small fraction (1% to 3%) of testosterone is unbound (free). This small fraction of free hormones exerts the effects. The liver produces SHBG. Estrogens stimulate hepatic produc-tion of SHBG. Greater estrogen production is associated with less free testosterone, whereas decreased estrogen pro-duction is associated with increased free testosterone. Therefore, measurement of total testosterone alone may not reflect the amount of biologically active testosterone.
Testosterone
receptors are scattered throughoutthe body. For the purpose
of this discussion, testosterone receptors are considered only in hair
follicles, sebaceous glands, and genital skin. Free testosterone enters the
cytosol of testosterone-dependent cells. There it is bound to a testosterone
receptor and carried into the nucleus of the cell to initiate its metabolic
action. When testosterone is exces-sive,
increased hair growth, acne, and rugation of the genital skin is seen. Some
individuals have increased 5α-reductasewithin
hair follicles, resulting in excessive local production of DHT.
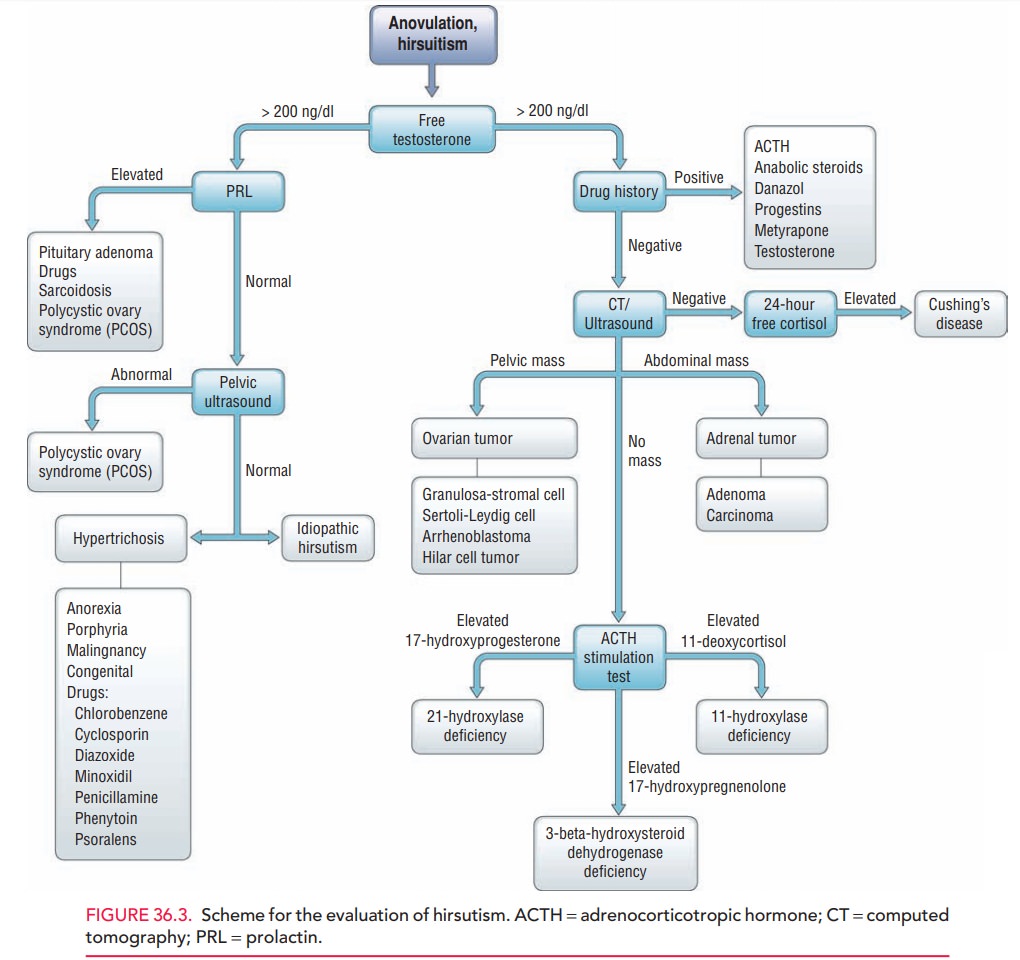
Excess androgen production has
several causes, includ-ing polycystic ovarian syndrome, testosterone-secreting
tumors, adrenal disorders, and iatrogenic and idiopathic causes. Figure 36.3
presents a scheme for the evaluation of hirsutism that encompasses the various
conditions that lead to this condition.
Related Topics