Chapter: Clinical Dermatology: Eczema and dermatitis
Allergic contact dermatitis
Allergic
contact dermatitis
Cause
The
mechanism is that of delayed (type IV) hyper-sensitivity. It has the following
features.
•
Previous contact is needed to induce
allergy.
•
It is specific to one chemical and
its close relatives.
•
After allergy has been established,
all areas of skin will react to the allergen.
•
Sensitization persists indefinitely.
•
Desensitization is seldom possible.
Allergens
In
an ideal world, allergens would be replaced by less harmful substances, and
some attempts are already being made to achieve this. A whole new industry has
arisen around the need for predictive patch testing before new substances or
cosmetics are let out into the community. Similarly, chrome allergy is less of
a problem now in enlightened countries that insist on adding ferrous sulphate
to cement to reduce its water-soluble chromate content. However, contact
allergens will never be abolished completely and family doctors still need to
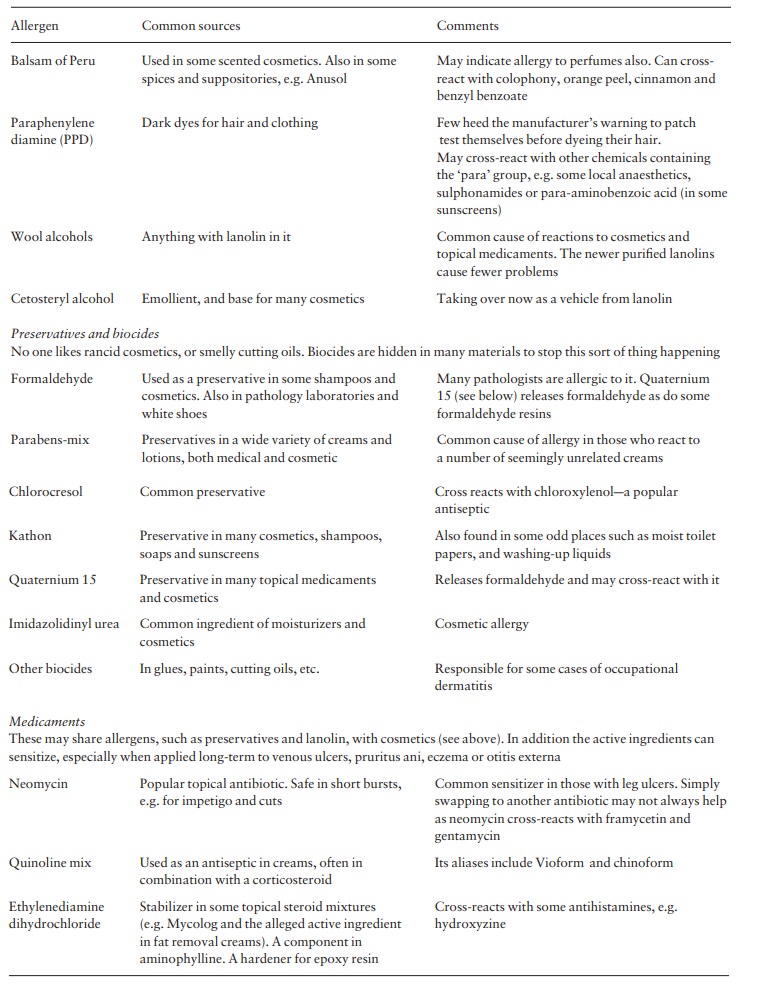
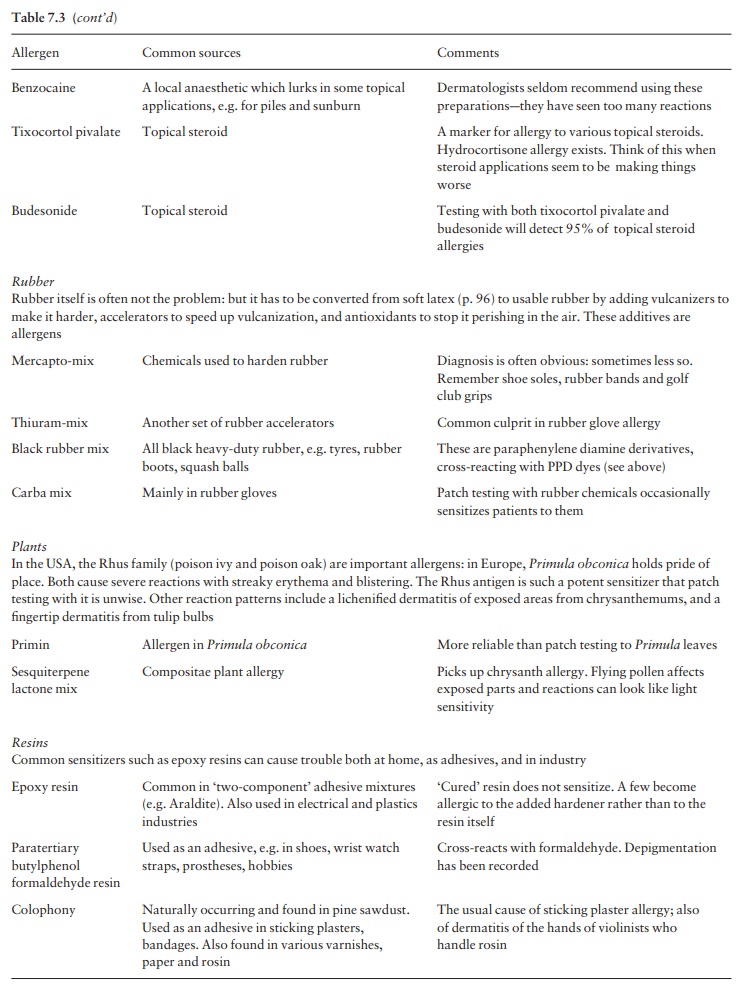
know about the most common ones and where to find them (Table 7.3). It is not
possible to guess which substances are likely to sensitize just by looking at
their formulae. In fact, most allergens are relatively simple chemicals that
have to bind to protein to become ‘complete’ anti-gens. Their ability to
sensitize variesafrom substances that can do so after a single exposure (e.g.
poison ivy), to those that need prolonged exposure (e.g. chromea bricklayers
take an average of 10 years to become allergic to it).
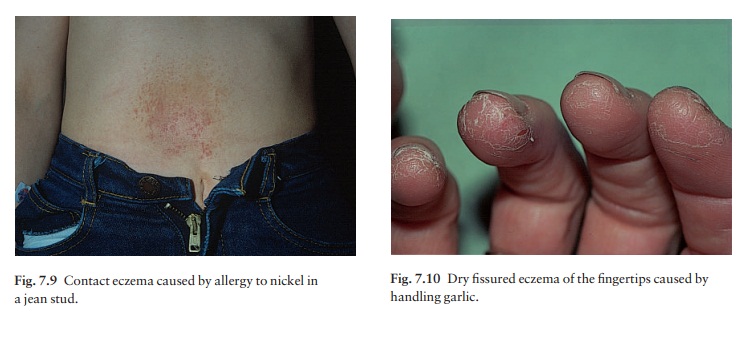
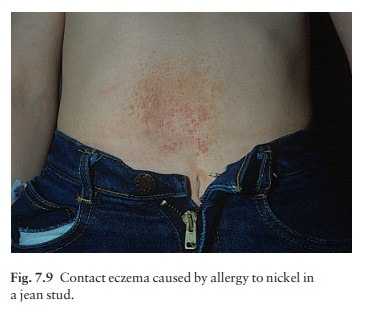
Presentation and clinical course
The original site of the eruption gives a clue to the likely allergen but secondary spread may later obscure this. Easily recognizable patterns exist. Nickel allergy, for example, gives rise to eczema under jewellery, braclips and jean studs (Fig. 7.9).
The lax skin of the eyelids and genitalia is
especially likely to become oedematous. Possible allergens are numerous and to
spot the less common ones in the environment needs specialist knowledge. Table
7.3 lists some common allergens and their distribution.
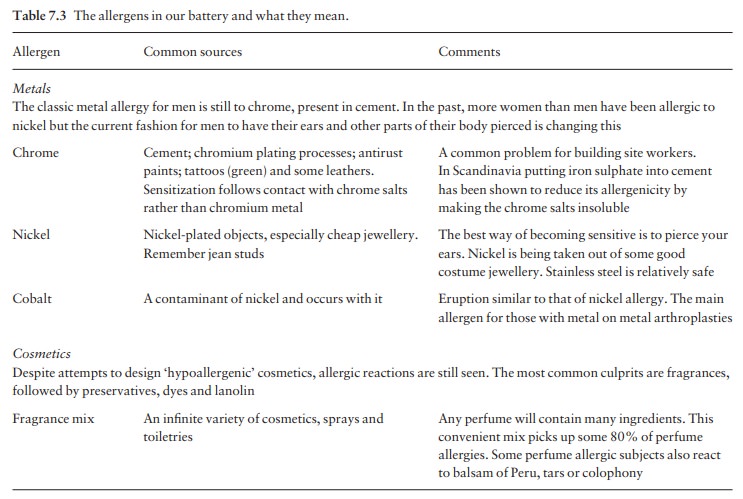
Allergic
contact dermatitis should be suspected if:
1 certain
areas are involved, e.g. the eyelids, external auditory meati, hands (Fig.
7.10) or feet, and around gravitational ulcers;
2 there is
known contact with the allergens mentionedin Table 7.3; or
3 the
individual’s work carries a high risk, e.g. hair-dressing, working in a flower shop,
or dentistry.

Investigations
Questioning
should cover both occupational and domestic exposure to allergens. The
indications for patch testing have already been discussed. Techniques are
constantly improving and derma-tologists will have access to a battery of
common allergens, suitably diluted in a bland vehicle. These are applied in
aluminium cups held in position on the skin for 2 or 3 days by tape. Patch
testing will often start with a standard series (battery) of allergens whose
selection is based on local experience. Table 7.3 shows the battery we use and
how it helps us with the most common types of contact allergy. This picks up
some 80% of reactions. Extra series of relevant allergens will be used for
problems such as hand eczema, leg ulcers and suspected cosmetic allergy, and
for those in jobs like dentistry or hairdressing, which carry unusual risks.
Some allergies are more common than others: in most centres, nickel tops the
list, with a positive reaction in some 15% of those tested; fragrance allergy
usually comes second. It is import-ant to remember that positive reactions are
not neces-sarily relevant to the patient’s current skin problem: some are
simply ‘immunological scars’ left behind by previous unrelated problems.
Treatment
Topical
corticosteroids give temporary relief, but far more important is avoidance of
the relevant allergen. Reducing exposure is usually not enough: active steps
have to be taken to avoid the allergen completely. Job changes are sometimes
needed to achieve this. Even then, other factors may come into play; e.g. some
believe that reactions to nickel can be kept going by nickel in the diet,
released from cans or steel saucepans, as changes in diet and cooking utensils
may rarely be helpful.
Related Topics