Chapter: Forensic Medicine: Toxicology and alcohol
Alcohol: Pharmacological effect
Pharmacological effect
General
The effect that alcohol has on the psyche, both
pleasant and unpleasant, is well-known. What is less well-known is that
alcohol, in different quantitiesfor different people, is a toxic drug. Alcohol
has both an acute and chronic effect on various organs of the body, including
the brain, heart, lungs, liver, the gastro-intestinal, genito-urinary and
endocrine systems.
a Nervous system
The damage that alcohol causes to the central
and peripheral nervous systems is of particular importance when it comes to the
driving of vehicles, as the following quote (Shaw: 1978) makes clear:
The exact mode of action of alcohol on the central nervous system is
unclear and its study complex. The effects of acute administration of alcohol
are often quite at variance with the effects of chronic administration and the
effects caused by a steady blood-alcohol level are often very different from
the effects caused by a changing blood-alcohol level. The rate of change may
itself be an important factor. Individual variation on whatever basis it may
rest is also important. Not only do we find that effects in the naõÈve subject
are very different from effects in the alcohol sophisticate, but it is well
known that all alcoholics do not suffer all the complications of alcoholism and
indeed some suffer none.
It appears that alcohol modifies the quality of
nerve-impulse transmission by stimulating the naturally occurring
nerve-transmission inhibitor, GABA, (gamma-amino-butyric acid) in the grey
matter of the brain. Drugs like Valium and barbiturates mimic this effect.
Similarly, cross-tolerance between these drugs and alcohol, when one of them is
used over a long period, is frequently observed. Furthermore, different types
of nerve cells display different degrees of sensitivity to the effects of
alcohol and these drugs.
The fact that we have stressed the complexity of
the effects of alcohol on the body should make it clear that many factors, as
yet poorly understood, could influence the response elicited by alcohol, and
that extreme caution should be exercised before expressing any final opinion on
individual behaviour and responses of the users of alcohol. In the early stages
of intoxication it is the loss of the inhibitory effect exercised by the higher
centres over the lower centres which accounts for the characteristic
behavioural changes such as the feeling of euphoria and the excessive
self-confidence which is out of all proportion to reality (Shaw: 1978).
It produces loss of emotional restraint and diminishes the inhibitions
which civilisation imposes on human conduct. Because in a social environment
many people become more active, both in speech and manner, it is widely (but
incorrectly) regarded as a stimulant.
The effect of alcohol on the nervous system is,
however, essentially depression of function, the extent of which depends on the
amount of alcohol working in on the brain cells, and the susceptibility of
these cells (or groups of cells) to alcohol. The cortical brain cells
(responsible for the higher functions) generally display the effect of alcohol
far sooner than those of the lower centres in the basal ganglia and the
midbrain. As blood-alcohol and thus brain-alcohol levels rise, more functions
of the nervous system are impaired, until co-ordination is drastically disturbed
and unconsciousness ensues. Deathcould follow due to depression of the
respiratory and later the circulatory control centres. It is said that alcohol
is in fact the most powerful depressant of the central nervous system that is
freely available without a doctor's prescription.
Furthermore, it seems as if alcohol prolongs
recovery time of the retinal response, and this is probably due to a direct
effect on the nerve cells of the retina.
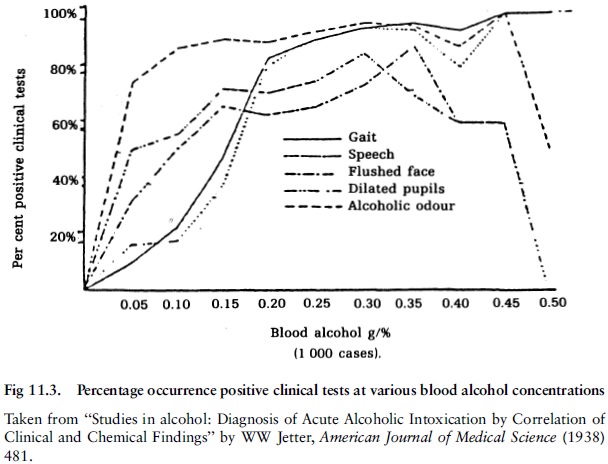
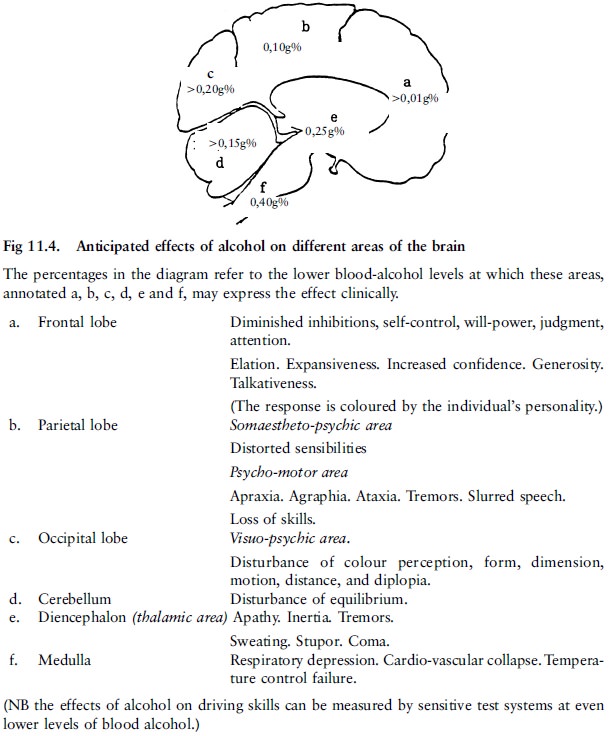
In broad terms it can be said that the effect of
alcohol on the highly developed frontal cortical regions of the brain
(responsible, inter alia, for conscious thought) can be seen with blood-alcohol
levels as low as 0,01%. This is manifested through altered judgment,
talkativeness and lack of attention (Shaw: 1978).
Early behavioural effects are much modified by personality factors in
the user and by the environmental situation in which drink is taken. In lively
company, disinhibition is the rule. The drinker becomes less self-conscious,
more talkative and less discreet. Judgment and restraint rapidly go and there
is loss of emotional control, giving rise to the humorous observation that the
super-ego is readily soluble in alcohol. As the blood level rises, thinking
becomes slowed and superficial and learning and retention become faulty. Less
attention is paid to stimuli so that internal stimuli such as hunger and pain
are ignored, sometimes with dire consequences. It becomes more difficult to
attend and respond to external stimuli. Events at the periphery are ignored and
only the immediate situation is given attention. This impaired psychological
state is usually accompanied by feelings of increased confidence and skill.
b Muscular system
The detrimental effect on muscle activity is due
to poor control by the central nervous system (and the decrease in impulse
conduction and transmission) over the use and co-ordination of muscle
potential, rather than to any direct impact on muscle strength itself.
Factors affecting pharmacological effect
The pharmacological effect of alcohol can be
modified by a number of congenital and acquired factors, which could partly
account for the different reactions of individuals to alcohol. One of these is
the elimination rate.
Certain organic, functional and degenerative
diseases could render the brain cells or parts of the brain more susceptible to
the intoxicating effect of alcohol. Severe liver disease, such as alcoholic
cirrhosis, can have a significant effect on the distribution and elimination of
drugs, including alcohol, and this makes it difficult to predict how such a
person will respond to alcohol or drugs in any dosage.
Degrees of intoxication: clinical features
(See also Kemp 1986:29±31.)
The clinical features of alcoholic intoxication
are mainly caused by its effect on the intellect, voluntary movement, speech
content, sensation, reflexes, cardio-vascular and gastrointestinal function.
It is customary to use various words and phrases
such as ``intoxicated'', ``under the influence'', ``drunk'' and ``paralytic''
to describe various states which may follow upon the consumption of alcohol.
These terms, as well as ``drunken driving'' and ``driving under the influence
of intoxicating liquor'' are at times used erroneously, as if they have the
same meaning.
It is suggested that the expression ``under the
influence'' be used to describe any abnormal mental or physical condition which
is the result of indulgence in any amount of alcohol, and which can range from
a state that deprives the subject of ``that clearness of intellect and control
which he would otherwise possess'' (Gradwohl 1954:971) to a state where death
from alcohol poisoning may be at hand. An individual under the influence of
alcohol could appear sober, that is, evidencing no noticeable effect at a
routine clinical examination, even to the skilled observer.
The clinically intoxicated person could
seemingly be:
·
lightly intoxicated
·
moderately intoxicated
·
heavily intoxicated
·
very heavily intoxicated
·
intoxicated to the extent of being stuporous to comatose
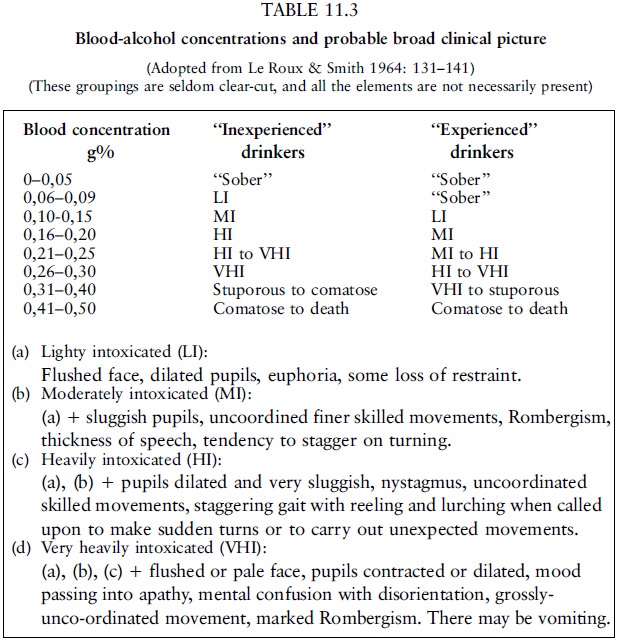
These degrees are not clearly distinguishable,
and rather represent a subtle progression of change in a broad spectrum of
behavioural and functional patterns. They tend to correspond broadly to
specific blood-alcohol concentrations, but wide variations are often seen
between the clinical picture and the BAC (blood alcohol concentration).
In individuals who are under the influence of
alcohol but appear sober, blood-alcohol levels of up to 0,08g% are often found.
Slight changes in neurological responses and behaviour compared to the
individual's normal responses may be detected by means of special tests not
normally used during the routine examinations, or by people who know the
subject well. The measured impairment detected by special tests is relative to
the subject's normal potential, and although not necessarily inferior to that
of another sober person, is nevertheless sufficient to materially affect
driving ability at levels of as low as 0,04g% or less.
a Lightly intoxicated
Clinically the subject may reveal signs of
mental impairment, unco-ordinated movements and speech defects. The face may be
flushed, the behaviour friendly, and the mood elevated. However, the reactions
are often coloured by the person's personality and surroundings. Euphoria or
depression, increased confidence, expansiveness, generosity, altered judgment
and absentmindedness may be present in differing degrees in different
individualsand in the same individual at different times at a given
blood-alcohol level. Clinical examinations generally reveal no other signs of
impairment. Blood-alcohol levels could reach 0,15g%. Subjectively the first
noticeable changes may be difficulty in visual accommodation and hearing,
especially when these functions are also impaired by disease or the ageing
process. The first movements to become visibly impaired are those requiring the
greatest skill.
b Moderately intoxicated
Clinical examination generally reveals evidence
of faculty impairment. The mood becomes less self-critical, and behavioural
changes, less tempered by reason, tend to be accentuated and often accompanied
by impulsive acts. The person is more reckless but sometimes also more
cautious. Unsteadiness when standing, turning and walking may be present in
varying degrees. Nystagmus (an involuntary rapid movement of the eyeball) is
usually present. The face is often flushed and the eyes bloodshot.
Blood-alcohol levels could reach 0,25g%, but generally range between 0,10 and
0,20g%.
c Heavily intoxicated
It is easy to detect functional impairment with
this degree of intoxication. Many aspects of behaviour are generally beyond
self-control and self-evaluation. The mind is dull and impairment of most
faculties is obvious. The faculties controlling the close co-ordination needed
for walking and other voluntary motor actions are markedly impaired.
Staggering, slurred and thick speech, the quality of which is shallow, confused
and illogical, is present. Movements are clumsy. Distance and position are
misjudged. The subject may attempt to conceal this impairment by performing
tasks more slowly. Pain and other sensations are dulled. Reflexes as tested
clinically are depressed and reaction time prolonged. The pupils become dilated
and react sluggishly to light. Co-ordination of eye movement is impaired.
Balance is impaired. Heart rate can increase. If nausea or vomiting is present,
the subject could be pale. Although intoxication is obvious to the observer,
the cause may (as in all degrees of intoxication) be difficult to determine. Blood-alcohol
levels of up to 0,30g% and very occasionally even higher are found.
d Very heavily intoxicated
There are confusion and disorientation with
regard to both time and place, apathy, drowsiness and marked disruption of both
motor and functional co-ordination. Confusion, disorientation and supressed
sensibility, particularly when accompanied by nausea and vomiting, could mask
or resemble underlying organic pathology. Blood-alcohol levels even in excess
of 0,35g% are found.
e Stuporous to comatose
It can be very difficult to determine the cause
of the stupor or coma. Unconsciousness, slow respiration, weak cardiac action
and dilated pupils with marked depression of all reflex reactions may be caused
by many different intoxicants and a great variety of diseases. Blood-alcohol
levels of up to 0,45g% and on rare occasions even higher may be found.
At levels of 0,45g% stupor is to be expected and
at levels of around 0,50g%, coma or death. Death has occurred at levels of
0,40g% or even lower in cold conditions, but recovery has occurred with levels
as high as 0,70g%. The manner of dying is via deepening coma to respiratory
paralysis.
In habitual drinkers the behavioural
disturbances will be less marked at all blood-alcohol levels, although it is
said that the alcoholic is no less susceptible than the non-alcoholic to
potentially lethal blood-alcohol levels. The well-known phenomenon of a
hangover (headache, fatigue and dizziness) can be caused by the alcohol or
acetaldehyde or both or by substances formed during the fermentation process.
It has also been suggested that most of the symptoms of a hangover can be the
result of hypoglycaemia. Blood-glucose levels are generally lower in both the
normal alcohol-naõÈve and the chronic alcoholic, but true hypoglycaemia is
rarely found the morning after.
In a recent study no correlation was found
between the impairment of psychomotor skills necessary for driving and the
intensity of the hangover, although irritability caused by the hangover could
lead to carelessness. Drugs, such as codeine compounds, taken to relieve the
symptoms of the hangover, could affect driving skill due to their psychoactive
effect.
Related Topics