Chapter: Biochemical Pharmacology : Pharmacodynamics
Toxic and beneficial drug effects
Toxic and beneficial drug
effects
As an anticlimactic finale to
this theory-heavy topic, let us consider the relationship between beneficial
(therapeutic) and toxic (side) effects of drugs. Possible forms of this
relationship are schematically depicted in Figure 3.13.
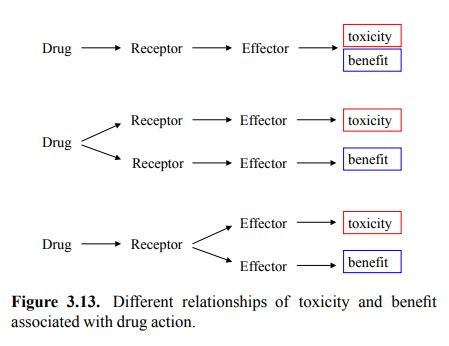
The first case applies if
toxicity arises simply as an exten-sion of the therapeutic effect. As an
example, consider war-farin, an inhibitor of an enzyme necessary in the
post-trans-lational modification of blood coagulation factors 9.
While it may help to prevent thrombosis and stroke when used in low amounts,
any excess in drug effect will be highly dan-gerous, leading to things such as
spontaneous hemorrhage into the brain.
Toxicity as an extension of
therapeutic action is usually as-sociated with a small therapeutic index, which is simply the ratio of the toxic plasma
concentration over the therapeutic plasma concentration. It should be apparent
that drugs with a small therapeutic index require the most attention and
alertness with respect to variations in metabolism and elim-ination. Such
variations may easily cause the concentration within the body to either exceed
the toxicity threshold, or drop below the minimum amount required for the
therapeu-tic effect. Accordingly, in our example, patients receiving warfarin
treatment need to have their blood clotting func-tion measured at regular,
frequent intervals.
In the second case in Figure
3.13, the therapeutic and the toxic effects are triggered from different
receptors alto-gether. The challenge then will be to find drugs that will
selectively act on the receptor responsible for the therapeu-tic action. As an
example, we may cite β-adrenergic recep-tors. The blockade of β receptors in the heart is used in the treatment of hypertension
and of heart disease; on the other hand, blockade of β receptors in the bronchi will promote bronchoconstriction and may
aggravate the symptoms of asthma. The β receptors in the heart mostly belong to the β1 subtype, whereas in the bronchi we mainly find β2 recep-tors. β1-Selective adrenergic antagonists ('cardioselective β blockers')
are available and preferably used in asthma patients.
In the third case Figure
3.13, the drug binds to a single re-ceptor alright, but the causal chains
leading to the thera-peutic and toxic effects, respectively, separate at a
point up-stream of the ultimate effectors. Inhibitors of monoamine oxidase may
serve as an example. Monoamine oxidase (MAO) is responsible for the degradation
of epinephrine and norepinephrine, dopamine, serotonin, and histamine.
Inhibition of this enzyme will therefore have a broad range of effects. To find
better therapeutic options, it would not seem useful to find `better inhibitors
10', but instead to try and find drugs acting downstream of the
branching point. In fact, MAO inhibitors are now obsolete and have been
su-perseded by drugs that act selectively on the receptors for the different
hormones.
Related Topics