Chapter: Medicine and surgery: Cardiovascular system
Thoracic aortic aneurysms and aortic dissection - Hypertension and vascular diseases
Thoracic aortic aneurysms and aortic dissection
Definition
Aortic dissection is defined as splitting through the endothelium and intima allowing the passage of blood into the aortic media.
Aetiology
Predisposing factors to thoracic aortic aneurysms, which may dissect include hypertension, atherosclerosis, bicuspid aortic valve, pregnancy, increasing age and MarfanŌĆÖs syndrome. In all cases there is degeneration of collagen and elastic fibres of the media, known as ŌĆścystic medial necrosisŌĆÖ. Trauma, including insertion of an arterial catheter, is also a cause.
Pathophysiology
There is an intimal tear, then blood forces into the aortic wall, it can then extend the split further along the wall of the vessel.
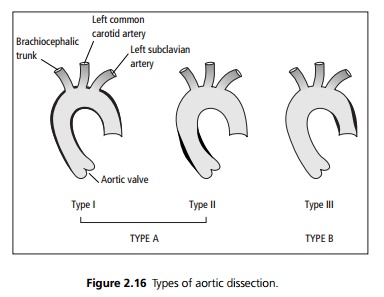
Type A dissections involve the ascending aorta (see Fig. 2.16), and in these cases the major risk is of dissection tracking back towards the heart, causing haemoperi-cardium and tamponade. These are further subdi-vided depending on whether the dissection extends beyond the brachiocephalic trunk (Type I) or not (Type II). Most thoracic aortic dissections are Type A, and these have the highest mortality.
Less commonly the dissection is confined to the descending aorta (Type B or Type III). The most common site for these to start is at the point of the ductus arteriosus, i.e. opposite to the left subclavian artery. Type I and Type III aortic dissections threaten the spinal arteries as well as the arteries supplying the abdominal viscera, e.g. mesenteric and coeliac axes and the renal arteries. They may extend as far down as the iliac arteries.
Clinical features
Dissection classically presents with excruciating sudden onset central chest pain, which may be mistaken for an acute myocardial infarction. The pain tends to be tearing, most severe at the onset and radiates through to the back. Most patients are hypertensive at presentation. Hypotension suggests significant blood loss, acute haemopericardium or disruption of the aortic valve. A difference in the blood pressure between the arms suggests impaired flow to one of the subclavian arteries. There may be reduction in the pulses distal to the lesion.
Auscultation may reveal the early diastolic murmur of aortic regurgitation and occasionally a pericardial rub. Haemorrhage from descending aortic aneurysms may cause dullness and absent breath sounds at the left lung base due to a left pleural effusion (haemothorax).
Complications
Dissection or formation of thrombus on the damaged endothelium may obstruct any branch of the aorta, and thus stroke, paraplegia (due to spinal artery involvement), renal failure and mesenteric ischaemia may result.
Investigations
ECG may be normal or show evidence of left ventricular hypertrophy due to long-standing hypertension. Myocardial infarction may occasionally be due to dissection involving the coronary arteries.
Chest X-ray may show a widened mediastinum: dilated aorta, an enlarged heart due to pericardial effusion and calcification of the aortic intima pushed further than normal within the aortic border.
The diagnosis is best confirmed with contrast CT or MR angiography. Transthoracic or transoesphageal echocardiography can give valuable information about the aorta and aortic valve, and may also be used to make the diagnosis, particularly in haemodynamically unstable patients.
Management
Dissection of the aorta is a medical (and surgical) emergency. In both types, urgent but careful resuscitation is required, and importantly hypertension should be treated, aiming at a maximal systolic blood pressure of 100ŌĆō120 mmHg to maintain renal and cerebral perfusion without exacerbating the dissection. Intravenous ╬▓-blockers, glyceryl trinitrate and hydralazine may all be needed. Adequate analgesia is required.
Type A dissections require emergency surgery with cardiopulmonary bypass. The ascending aorta is replaced using a Dacron graft and the aortic valve re-paired or replaced as necessary. The aortic arch and its branches may also need repair or replacement.
Type B dissections should be treated conservatively with antihypertensive therapy. Surgery or endovascular stenting may be indicated if the dissection progresses, or if rupture occurs, but the risk of paraplegia due to spinal artery ischaemia during surgery is high.
Asymptomatic thoracic aortic aneurysms found by screening, e.g. in MarfanŌĆÖs syndrome, are closely monitored with echocardiograms and CT scans for expansion and may be treated electively by surgical repair.
Prognosis
Untreated thoracic aortic dissection results in 50% mortality within 48 hours. In all patients long-term strict blood pressure control is needed.
Related Topics