Chapter: Medical Physiology: Adrenocortical Hormones
Renal and Circulatory Effects of Aldosterone
Renal and Circulatory Effects of Aldosterone
Aldosterone Increases Renal Tubular Reabsorption of Sodium and Secretion of Potassium. It will be recalled that aldosterone increases absorption of sodium and simultaneously increases secretion of potassium by the renal tubular epithelial cells especially in the principal cells of the collecting tubules and, to a lesser extent, in the distal tubules and col-lecting ducts. Therefore, aldosterone causes sodium to be conserved in the extracellular fluid while increasing potassium excretion in the urine.
A high concentration of aldosterone in the plasma can transiently decrease the sodium loss into the urine to as little as a few milliequivalents a day. At the same time, potassium loss into the urine increases several-fold. Therefore, the net effect of excess aldosterone in the plasma is to increase the total quantity of sodium in the extracellular fluid while decreasing the potassium.
Conversely, total lack of aldosterone secretion can cause transient loss of 10 to 20 grams of sodium in the urine a day, an amount equal to one tenth to one fifth of all the sodium in the body. At the same time, potas-sium is conserved tenaciously in the extracellular fluid.
Excess Aldosterone Increases Extracellular Fluid Volume and Arterial Pressure but Has Only a Small Effect on Plasma Sodium Concentration. Although aldosterone has a potenteffect in decreasing the rate of sodium ion excretion by the kidneys, the concentration of sodium in the extracellular fluid often rises only a few milliequiva-lents. The reason for this is that when sodium is reab-sorbed by the tubules, there is simultaneous osmotic absorption of almost equivalent amounts of water. Also, small increases in extracellular fluid sodium concentration stimulate thirst and increased water intake, if water is available. Therefore, the extracellu-lar fluid volume increases almost as much as the retained sodium, but without much change in sodium concentration.
Even though aldosterone is one of the body’s most powerful sodium-retaining hormones, only transient sodium retention occurs when excess amounts are secreted. An aldosterone-mediated increase in extra-cellular fluid volume lasting more than 1 to 2 days also leads to an increase in arterial pressure. The rise in arterial pressure then increases kidney excretion of both salt and water, called pressure natriuresis and pressure diuresis, respectively. Thus, after the extracellular fluid volume increases 5 to 15 per cent above normal, arterial pres-sure also increases 15 to 25 mm Hg, and this elevated blood pressure returns the renal output of salt and water to normal despite the excess aldosterone (Figure77–3).
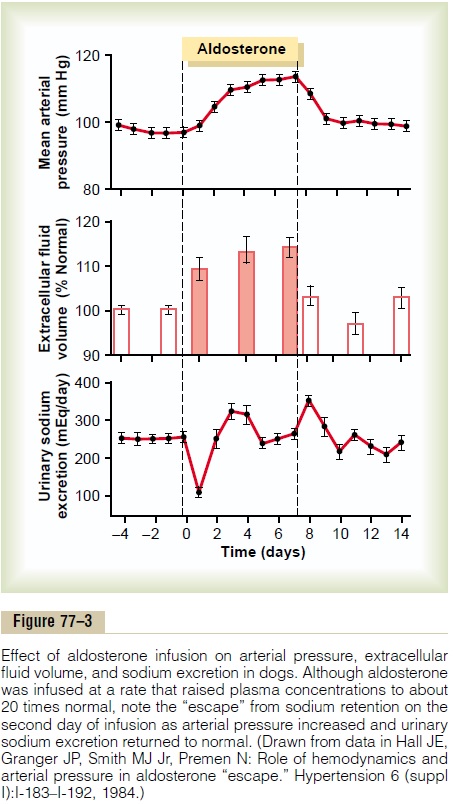
This return to normal of salt and water excretion by the kidneys as a result of pressure natriuresis and diuresis is called aldosterone escape. Thereafter, the rate of gain of salt and water by the body is zero, and balance is maintained between salt and water intake and output by the kidneys despite continued excess aldosterone. In the meantime, however, the person has developed hypertension, which lasts as long as the person remains exposed to high levels of aldosterone.
Conversely, when aldosterone secretion becomes zero, large amounts of salt are lost in the urine, not only diminishing the amount of sodium chloride in the extracellular fluid but also decreasing the extracellular fluid volume. The result is severe extracellular fluid dehydration and low blood volume, leading to circula-tory shock. Without therapy, this usually causes deathwithin a few days after the adrenal glands suddenly stop secreting aldosterone.
Excess Aldosterone Causes Hypokalemia and Muscle Weak-ness; Too Little Aldosterone Causes Hyperkalemia and Cardiac Toxicity. Excess aldosterone not only causes loss ofpotassium ions from the extracellular fluid into the urine but also stimulates transport of potassium from the extracellular fluid into most cells of the body. Therefore, excessive secretion of aldosterone, as occurs with some types of adrenal tumors, may cause a serious decrease in the plasma potassium concentration, sometimes from the normal value of 4.5 mEq/L to as low as 2 mEq/L. This condition is called hypokalemia. When the potassium ion concen-tration falls below about one-half normal, severe muscle weakness often develops. This is caused by alteration of the electrical excitability of the nerve and muscle fiber membranes, which pre-vents transmission of normal action potentials.
Conversely, when aldosterone is deficient, the extra-cellular fluid potassium ion concentration can rise far above normal.When it rises to 60 to 100 per cent above normal, serious cardiac toxicity, including weakness of heart contraction and development of arrhythmia, becomes evident; progressively higher concentrations of potassium lead inevitably to heart failure.
Excess Aldosterone Increases Tubular Hydrogen Ion Secretion, and Causes Mild Alkalosis. Aldosterone not only causespotassium to be secreted into the tubules in exchange for sodium reabsorption in the principal cells of the renal collecting tubules but also causes secretion of hydrogen ions in exchange for sodium in the interca-lated cells of the cortical collecting tubules. Thisdecreases the hydrogen ion concentration in the extra-cellular fluid, causing a mild degree of alkalosis.
Related Topics