Chapter: Clinical Dermatology: Other papulosquamous disorders
Pityriasis rosea
Pityriasis
rosea
Cause
The
cause of pityriasis rosea is not known. An infec-tious agent has always seemed
likely but has not yet been proven: human herpesvirus 7 is the latest sus-pect.
The disorder seems not to be contagious.
Presentation
Pityriasis
rosea is common, particularly during the winter. It mainly affects children and
young adults,
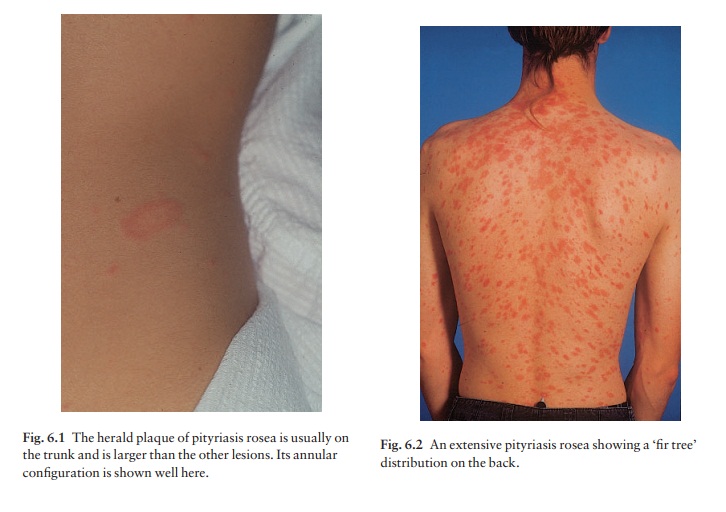
Most patients develop one plaque (the ‘herald’ or
‘mother’ plaque) before the others (Fig. 6.1). It is larger (2–5 cm in
diameter) than later lesions, and is rounder, redder and more scaly. After
several days many smaller plaques appear, mainly on the trunk, but some also on
the neck and extremities. About half of the patients complain of itching. An
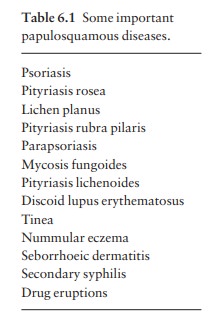
individual plaque is oval, salmon pink and shows a delicate scaling, adherent
peripherally as a collarette. The configuration of such plaques is often
characteristic. Their longitudinal axes run down and out from the spine (Fig.
6.2), along the lines of the ribs. Purpuric lesions are rare.


Course
The
herald plaque precedes the generalized eruption by several days. Subsequent
lesions enlarge over the first week or two. A minority of patients have
systemic symptoms such as aching and tiredness. The erup-tion lasts between 2
and 10 weeks and then resolves spontaneously, sometimes leaving hyperpigmented
patches that fade more slowly.
Differential diagnosis
Although
herald plaques are often mistaken for ringworm, the two disorders most likely
to be mis-diagnosed early in the general eruption are guttate psoriasis and
secondary syphilis. Tinea corporis and pityriasis versicolor can be
distinguished by the micro-scopical examination of scales, and secondary
syphilis by its other features (mouth lesions, palmar lesions, condyloma lata,
lymphadenopathy, alopecia) and by serology. Gold and captopril are the drugs
most likely to cause a pityriasis rosea-like drug reaction, but barbiturates,
penicillamine, some antibiotics and other drugs can also do so.
Investigations
Because
secondary syphilis can mimic pityriasis rosea so closely, testing for syphilis
is usually wise.
Treatment
No
treatment is curative, and active treatment is seldom needed. A moderately
potent topical steroid or calamine lotion will help the itching. One per cent
salicylic acid in soft white paraffin or emulsifying oint-ment reduces scaling.
Sunlight or artificial UVB often relieves pruritus and may hasten resolution.
Related Topics