Chapter: Clinical Dermatology: Other papulosquamous disorders
Parapsoriasis and premycotic eruption
Parapsoriasis
and premycotic eruption
Parapsoriasis
is a contentious term, which many would like to drop. We still find it useful
clinically for lesions that look a little like psoriasis but which scale subtly
It is worth
trying to distinguish a benign type of parapsoriasis from a premycotic type,
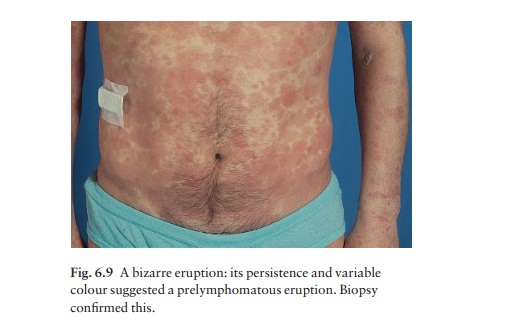
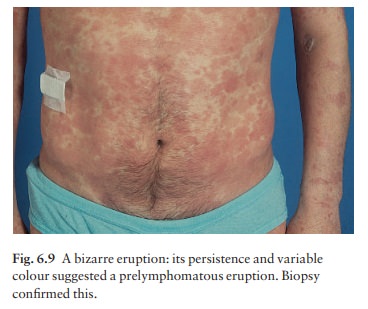
which is a forerunner of mycosis fungoides, a cutaneous T-cell lymphoma (Fig.
6.9)aalthough they can look alike early in their development. However, even the
term ‘premycotic’ is disputed, as some think that these lesions are mycosis
fungoides right from the start, preferring the term ‘patch stage cutaneous
T-cell lymphoma’.
Cause
The
cause is otherwise unknown.
Presentation
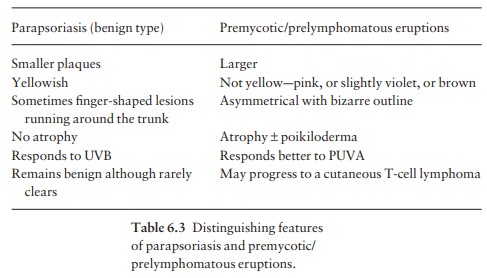
Pink scaly well-marginated plaques appear, typically on the buttocks, breasts, abdomen or flexural skin. The distinguishing features of the small-plaque (benign) and large-plaque (premycotic/prelymphomatous) types are given in Table 6.3.
Perhaps the most important point
to look for is the presence of poikiloderma (atrophy, telangiectasia and
reticulate pigmentation) in the latter type. Both conditions are stubborn in
their response to topical treatment, although often responding temporarily to
PUVA. Itching is variable.
Complications
Patients with suspected premycotic/prelymphomatous eruptions should be followed up carefully, even though the development of cutaneous T-cell lymphoma may not occur for years. If poikiloderma or induration develops, the diagnosis of a cutaneous T-cell lym-phoma becomes likely
Differential diagnosis
This
includes psoriasis, tinea and nummular (discoid) eczema. In contrast to
psoriasis and pityriasis rosea, the lesions of parapsoriasis,
characteristically, are asymmetrical. Topical steroids can cause atrophy and
confusion.
Investigations
Several
biopsies should be taken if a premycotic erup-tion is suspected, if possible
from thick or atrophic untreated areas. These may suggest an early cutaneous
T-cell lymphoma, with bizarre mononuclear cells both in the dermis and in
microscopic abscesses within the epidermis. Electron microscopy may show
abnormal lymphocytes with convoluted nuclei in the dermis or epidermis, although
the finding of these cells, especially in the dermis, is non-specific. DNA
probes can determine monoclonality of the T cells within the lymphoid
infiltrate of mycosis fungoides based on rearrangements of the T-cell receptor
genes. The use of these probes and of immunophenotyping
Treatment
Treatment
is controversial. Less aggressive treatments are used for the benign type of
parapsoriasis. Usually, moderately potent steroids or ultraviolet radiation
bring some resolution, but lesions tend to recur when these are stopped. For
premycotic/prelymphomatous eruptions, treatment with PUVA with topi-cal nitrogen mustard paints, is
advocated by some, although it is not clear that this slows down or pre-vents
the development of a subsequent cutaneous T-cell lymphoma.
Related Topics