Chapter: Modern Pharmacology with Clinical Applications: Hypocholesterolemic Drugs and Coronary Heart Disease
Management of Hyperlipidemias With Drugs: Other Hypocholesterolemic Drugs
Other Hypocholesterolemic Drugs
Resins
Mechanism of Action
Prior to the introduction of
the statins in the mid to late 1980s, the bile acid–sequestering drugs
cholestyra-mine (Questran) and
colestipol (Colestid) were primary
drugs for lowering plasma cholesterol. Today they are second-line drugs that
can safely be given with a statin to enhance cholesterol lowering or as an
alternative for patients intolerant to a statin or concerned with statin’s
potential for toxicity. Alone, the resins can achieve 20 to 25% reductions in
LDL cholesterol, but when used with a statin, such as lovastatin, reductions of
50% and more can be seen.
These drugs are basically
anion exchange resins that remain in the gut, bind intestinal bile acids, and
greatly increase their fecal excretion (mechanism I in Fig. 23.2).

The lowered concentration of
bile acids returning to the liver by the enterohepatic circulation results in
dere-pression of 7- -hydroxylase, the rate-limiting enzyme for conversion of
cholesterol to bile acids. This results in increased use of cholesterol to
replace the excreted bile acids and lowering of hepatic cholesterol (mechanism
VI in Fig. 23.2). Thus, similar to the statins, the ultimate actions of the
bile acid–sequestering resins are up-regulation of transcription of the LDL
receptor gene, increased hepatic receptor activity, and lowering of plasma LDL
cholesterol (mechanism VII in Fig. 23.2).
Clinical Uses
The bile acid sequestering
resins lower elevated LDL cholesterol and therefore are useful in the
treat-ment of type IIa hyperlipoproteinemia. However, be-cause the resins can
raise plasma VLDL in some pa-tients, they are not recommended for treatment of
combined hyperlipidemias (type IIb) when both LDL cholesterol and VLDL triglycerides
are high or in other conditions of elevated triglycerides.
Adverse Effects
The resins are interesting
drugs because they have profound metabolic effects without truly entering the
body. Perhaps for this reason they are relatively safe, with constipation being
the chief complaint. Because the resins are given as the chloride salt and the
chloride is exchanged for the negatively charged bile salt, bile acid resins
can lead to hyperchloremic acidosis in vulnerable patients (children and
patients with kidney failure).
Drug Interactions
The principal precaution with
use of the bile acid resins is the possibility of impaired absorption of other
drugs given orally at the same time. Cholestyramine and colestipol can bind
many other drugs, such as digitoxin, phenobarbital, chlorothiazide, and
warfarin, and delay or prevent their absorption. For this reason, other drugs
should always be taken at least 1 hour before or 4 to 6 hours after the resin.
The resins can also decease ab-sorption of fat-soluble vitamins.
Nicotinic Acid (Niacin)
Nicotinic acid has three
special features as a hypolipi-demic drug: it has multiple beneficial effects
on serum lipoproteins, it is the least expensive, and it is the least well
tolerated.
Mechanism of Action
Nicotinic acid decreases
formation and secretion of VLDL by the liver (mechanism III in Fig. 23.2). This
ac-tion appears secondary to its ability to inhibit fatty acid mobilization
from adipose tissue. Circulating free fatty acids provide the main source of
fatty acids for hepatic triglyceride synthesis, and lowering triglyceride
synthe-sis lowers VLDL formation and secretion by the liver. Since plasma VLDL
is the source of LDL, lowering VLDL can ultimately lower LDL. In addition,
nicotinic acid shifts LDL particles to larger (more buoyant) sizes. The larger
LDL particles are thought to be less athero-genic. Nicotinic acid can also
significantly increase plasma HDL levels; the mechanism is unknown.
Clinical Uses
Used alone, nicotinic acid
can decrease plasma LDL cholesterol levels by 15 to 30%. It can also be used in
combination therapy with the statins or the bile acid– sequestering resins to
augment reduction of very high LDL levels. Because nicotinic acid can lower
plasma triglycerides by 40% or more, it is useful in treating fa-milial
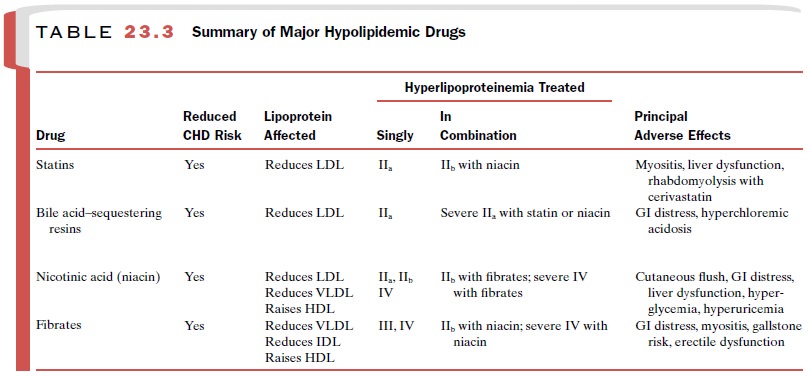
hypertriglyceridemia type IV (Table 23.3), and in combination with the statins
it is useful in treating com-bined hyperlipidemia type IIb. As described later
with the fibrates, patients with high plasma triglycerides plus low HDL are at
increased risk for CHD. Nicotinic acid is useful for treating these patients,
since it can both lower triglycerides and raise HDL.
Adverse Effects
Compliance with nicotinic
acid therapy can be poor because the drug can produce an intense cutaneous
flush. This can be reduced by beginning the drug in stepped doses of 250 mg
twice daily and increasing the dose monthly by 500 to 1000 mg per day to a
maximum of 3000 mg per day. Taking nicotinic acid on a full stom-ach (end of
meal) and taking aspirin before dosage can reduce the severity of flushing.
Time-release forms of nicotinic acid may also decrease cutaneous flushing.
Nicotinic acid can cause gastrointestinal (GI) distress, liver dysfunction
(especially at high doses), decreased glucose tolerance, hyperglycemia, and
hyperuricemia. Thus, it is contraindicated in patients with hepatic
dys-function, peptic ulcer, hyperuricemia, or diabetes melli-tus. A paradox
associated with nicotinic acid is that it is the most widely available
hypolipidemic drug (it is sold over the counter), yet its use requires the
closest man-agement by the physician.
Related Topics