Chapter: Basic Radiology : Plain Film of the Abdomen
Exercise: Increased or Decreased Density in the Abdomen
EXERCISE 8-5.
INCREASED OR DECREASED DENSITY IN THE ABDOMEN
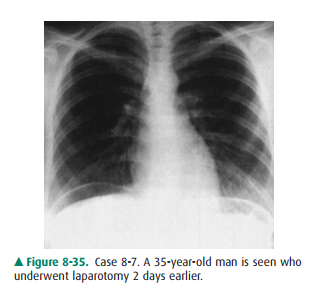
8-17. What is the most
likely diagnosis in Case 8-17
(Figure8-35)?
A.
Bullous emphysema
B.
Colon interposition
C.
Pneumoperitoneum
D.
Tension pneumothorax
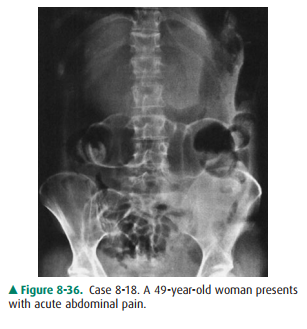
8-18. What is the most
likely diagnosis in Case 8-18 (Figure8-36)?
A.
Functional ileus of the bowel
B.
Mechanical obstruction of the colon
C.
Mechanical obstruction of the small bowel
D.
Pneumoperitoneum
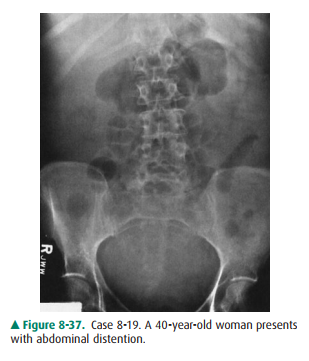
8-19. What is the most
likely diagnosis in Case 8-19 (Figure8-37)?
A.
Ascites
B.
Functional ileus
C.
Gallstone ileus
D.
Mechanical obstruction in the small bowel
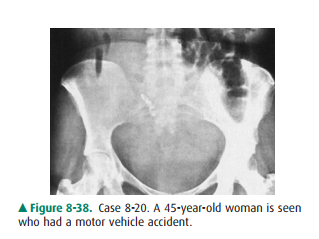
8-20. What is the most
likely diagnosis in Case 8-20 (Figure8-38)?
A.
Ascites
B.
Hemoperitoneum
C.
Pelvic teratoma
D.
Uterine fibroma.
Radiologic
Findings
8-17. This case shows crescent-shaped lucencies beneath both hemidiaphragms outline the liver on the rightand the spleen
on the left in the PA chest film, suggesting pneumoperitoneum (C is the correct
answer to Question 8-17).
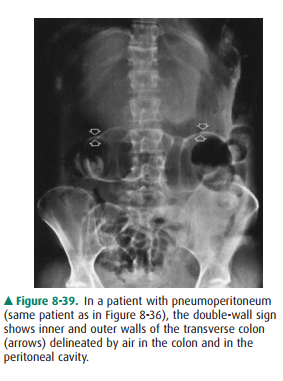
8-18. This case shows both the inner and outer walls of the transverse colon (arrows)
(Figure 8-39). This double-wall sign is seen on the supine film of the ab-domen
because there is air within the intestinal lumen and in the peritoneal cavity,
caused by rupture of a viscus (D is the correct answer to Question 8-18).
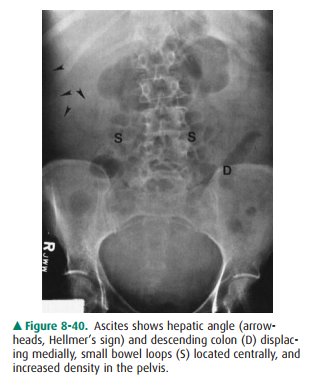
8-19.In this case, the hepatic angle (arrowheads) and the descending
colon (D) are displaced medially, the small bowel (S) is located centrally in
the abdomen, and there is increased density in the pelvis, suggesting ascites
(Figure 8-40) (A is the correct answer to Ques-tion 8-19).
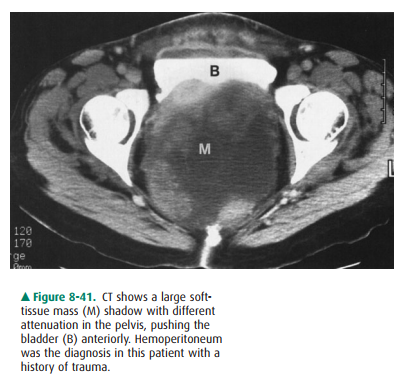
8-20.In this case, the soft-tissue density with no gas pat-tern in
the pelvis is consistent with hemoperitoneum in this motor vehicle accident
victim. CT better eval-uates hemoperitoneum (Figure 8-41) (B is the cor-rect
answer to Question 8-20).
Discussion
In adults, the most common causes
of pneumoperitoneum are postoperative status, ruptured abdominal viscus, and
peritoneal dialysis. Residual air in the abdomen after surgery may persist for
1 to 2 weeks. Serial abdominal films, however, should show a gradual reduction
in the amount of free peri-toneal air. A persistent or increasing amount of air
on post-operative serial films suggests a perforated viscus or ruptured
surgical anastomosis. Spontaneous pneumoperitoneum is commonly caused by the
perforation of a duodenal ulcer. Less common causes include pneumomediastinum,
pul-monary emphysema, pneumatosis intestinalis, and entrance of air per vagina.
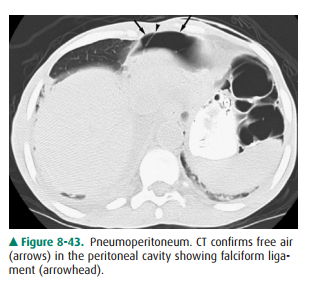
Pneumoperitoneum is most readily
detected on the up-right film of the chest, even if only a small amount of air
is present. The left lateral decubitus view is useful and may show small amount
of free air accumulating between the right lateral margin of the liver and the
peritoneal surface. Normally, the interface between the air and inner
intestinal wall is visible, but the serosal surface is not appreciated be-cause
its density is similar to that of the adjacent peritoneal contents. When gas is
present in the peritoneal cavity, how-ever, both inner and outer walls will be
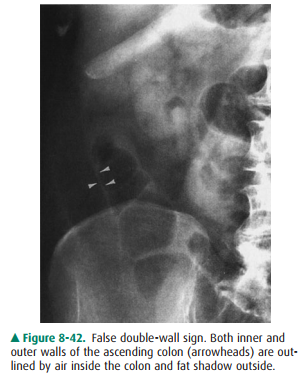
delineated; this is called the “double-wall sign” or “Rigler’s sign”. A visible
serosal margin of bowel can also be simulated by normal adjacent omental fat or
adjacent contiguous loops of small or large bowel (Figure 8-42). If in doubt,
the upright or left lateral decubitus film may confirm pneumoperitoneum. CT is
more sensitive than plain radiograph in assessing pneu-moperitoneum (Figure
8-43). Colon interposition occurs on the right between the liver and
hemidiaphragm, and haustrations are usually recognized that aid differentiation
from pneumoperitoneum.
Although plain film of the
abdomen is not sensitive in assessing small amounts of intraperitoneal fluid,
the plain film can demonstrate moderate and large amounts of fluid collection.
In ascites, the hepatic angle may be obscured ordisplaced medially (Hellmer’s
sign). The ascending or de-scending colon may be displaced medially by fluid in
the paracolic gutter. A large amount of fluid may accumulate in the pelvis,
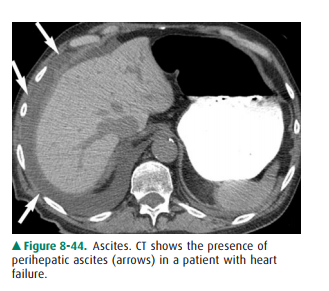
causing increased density and symmetrical bulges. Other signs, such as
separation of the small bowel loops and overall higher density in the abdomen,
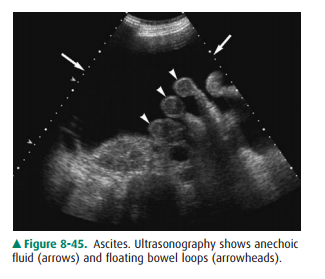
are also seen, but not often. CT (Figure 8-44) and ultrasonography (Figure
8-45) more accurately assess intraperitoneal fluid and coexistent masses.
Blood and pus have a similar
density to that of ascitic fluid in the peritoneal cavity; therefore,
hemoperitoneum mayproduce signs similar to those found in ascites. High density
in the pelvis is a sign of hemoperitoneum in patients with a history of trauma.
CT better evaluates hemoperitoneum.
Related Topics