Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Herpesviruses
Varicella - Zoster Disease : Clinical Aspects
VARICELLA – ZOSTER DISEASE : CLINICAL ASPECTS
MANIFESTATIONS
VZV produces a primary infection in normal children characterized by a generalized vesicular rash termed chickenpox or varicella. After clinical infection resolves, the virus persists for decades in the absence of clinical manifestation. Chickenpox lesions gener-ally appear on the back of the head and ears, then spread centrifugally to the face, neck, trunk, and proximal extremities. Involvement of mucous membranes is common, and fever may occur early in the course of disease. Lesions appear in different stages of evo-lution; this characteristic is one of the major features used to differentiate varicella from smallpox, in which lesions are concentrated on the extremities and all had a similar ap-pearance. Varicella lesions are pruritic (itchy), and the number of lesions may vary from 10 to several hundred.
Immunocompromised children may develop progressive varicella, which is associated with prolonged viremia and visceral dissemination as well as pneumonia, encephalitis, hepatitis, and nephritis. Progressive varicella has an estimated mortality of approximately 20%. In thrombocytopenic patients, the lesions may be hemorrhagic. Susceptible adults are at higher risk (15 x ) for VZV pneumonia during chickenpox.
Reactivation of VZV is associated with the disease herpes zoster (shingles). Although zoster is seen in patients of all ages, it increases in frequency with advanc-ing age. Clinically, pain in a sensory nerve distribution may herald the onset of the eruption, which occurs several days to a week or two later. The vesicular eruption is usually unilateral, involving one to three dermatomes. New lesions may appear over the first 5 to 7 days. Multiple attacks of VZV infection are uncommon; if recurrent at-tacks of a vesicular eruption occur in one area of the body, HSV infection should be considered.
The complications of VZV infection are varied and depend on age and host immune factors. Postherpetic neuralgia is a common complication of herpes zoster in elderly adults. It is characterized by persistence of pain in the dermatome for months to years af-ter resolution of the lesions of zoster and appears to result from damage to the involved nerve root. Immunosuppressed patients may develop localized zoster followed by dissem-ination of virus with visceral infection, which resembles progressive varicella. Bacterial superinfection is also possible. Maternal varicella infection during early pregnancy can result in fetal embryopathy with skin scarring, limb hypoplasia, microcephaly, cataracts, chorioretinitis, and microphthalmia. Severe varicella can also occur in seronegative neonates, with mortality as high as 30%.
DIAGNOSIS
Varicella or herpes zoster lesions can be diagnosed clinically, although they may occa-sionally be difficult to distinguish from those caused by HSV or even vaccinia smallpox. Scrapings of lesions may reveal multinucleated giant cells characteristic of herpesviruses, but cytologic examination does not distinguish HSV lesions from those due to VZV. For rapid viral diagnosis, the best procedure is to demonstrate varicella–zoster antigen in cells from lesions by immunofluorescent antibody staining. VZV can be isolated from vesicu-lar fluid or cells inoculated onto human diploid fibroblasts; however, the virus is difficult to grow from zoster (shingles) lesions older than 5 days, and cytopathic effects are usually not seen for 5 to 9 days. PCR of CSF may be useful in the diagnosis of VZV en-cephalitis; culture is rarely positive.
TREATMENT
Acyclovir has been shown to reduce fever and skin lesions in patients with varicella, and its use is recommended in healthy patients over 18 years of age. There are insufficient data to justify universal treatment of all healthy children and teenagers with varicella. In immunosuppressed patients, controlled trials of acyclovir have been effective in reducing dissemination, and the use of this agent is definitely indicated. In addition, controlled trials of acyclovir have demonstrated effectiveness in the treatment of herpes zoster in immunocompromised patients. Acyclovir may be used to treat herpes zoster in immuno-competent adults, but it appears to have only a modest impact on the development of post-herpetic neuralgia, the most important complication of zoster. Treatment should be started within 3 days of the onset of zoster. VZV is less susceptible than HSV to acyclovir, so the dosage for treatment is substantially higher. Famciclovir or valacyclovir are more convenient and may be more effective.
PREVENTION
High-titer immune globulin administered within 96 hours of exposure is useful in pre-venting infection or ameliorating disease in patients at risk for severe primary infection (eg, immunosuppressed children who are household or play contacts of patients with vari-cella or zoster). Once skin lesions have occurred, high-titer immune globulin has not proved useful in ameliorating disease or preventing dissemination. Immune globulin is not indicated for the treatment or prevention of reactivation (ie, zoster or shingles). In nonimmunosuppressed children, varicella is a relatively mild disease, and passive immu-nization is not indicated.
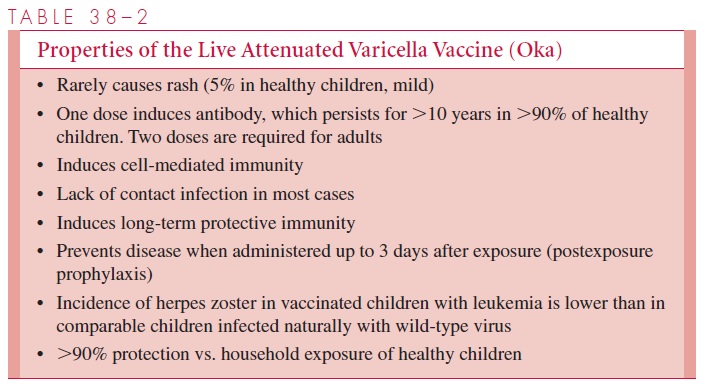
A live vaccine developed by a group of Japanese workers appears to be effective in both immunosuppressed and immunocompetent persons and is now recommended for routine use after 12 months of age in healthy children (Table 38–2). In immunocompro-mised patients who are susceptible to varicella, chickenpox can be extremely serious, even fatal. In these patients, the live vaccine appears to be protective although it is not ap-proved for this use in the United States. The vaccine is being used routinely in immuno-competent seronegative adults, especially those at occupational risk, such as health care workers, and it can even be helpful if given to a seronegative, immunocompetent adult shortly after exposure. Varicella is a highly contagious disease, and rigid isolation precau-tions must be instituted in all hospitalized cases.
Related Topics