Chapter: Medical Surgical Nursing: Health Education and Health Promotion
The Nature of Teaching and Learning
The Nature of Teaching and Learning
Learning can be defined as acquiring knowledge,
attitudes, orskills. Teaching is defined as helping another person to learn.
These definitions indicate that the teaching–learning process is an active one,
requiring the involvement of both teacher and learner in the effort to reach
the desired outcome, a change in behavior. The teacher does not simply give
knowledge to the learner, but instead serves as a facilitator of learning.
In general, there is no
definitive theory about how learning oc-curs and how it is affected by
teaching. However, learning can be affected by factors such as readiness to
learn, the learning envi-ronment, and the teaching techniques employed
(Bastable, 1997; Green & Kreuter, 1999).
LEARNING READINESS
One of the most significant factors influencing learning is the per-son’s learning readiness. For adults, readiness is based on culture, personal values, physical and emotional status, and past experiences in learning. The teachable moment for an adult occurs when the content and skills being taught are congruent with the task to be accomplished (Redman, 2000).
Culture encompasses
values, ideals, and behaviors, and the tra-ditions within each culture provide
the framework for solving the issues and concerns of daily living. Because
people with different cultural backgrounds hold different values, lifestyles
and choices about health care vary. Culture is a major variable influencing
readiness to learn because it affects how a person learns and what information
can be learned. Sometimes people will not accept health teaching because it
conflicts with culturally mediated values. Before beginning health teaching,
the nurse must perform an in-dividual cultural assessment instead of relying
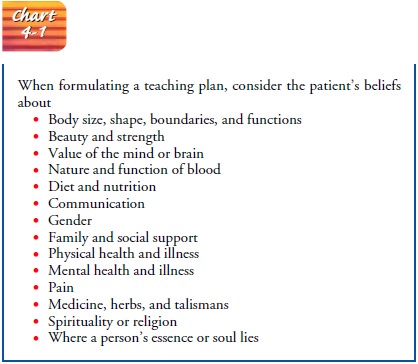
only on generalized assumptions about a particular culture. A patient’s social
and cultural patterns must be appropriately incorporated into the
teaching–learning interaction. Chart 4-1 describes cultural assess-ment
components to consider when formulating a teaching plan.
An individual’s values
include beliefs about what are desirable and undesirable behaviors. The nurse
must know what value the patient places on health and health care. In clinical
situations, pa-tients express their values through the actions performed and
the level of knowledge pursued (Andrews & Boyle, 1998). When the nurse
lacks knowledge about the cultural values of the patient being instructed,
misunderstanding, lack of cooperation, and negative health outcomes may occur
(Leininger, 1991). Each per-son’s values and behaviors can be either an asset
or a deficit to the readiness to learn. Therefore, no amount of health
education will be accepted by patients unless their values and beliefs about
health and illness are respected (Giger & Davidhizar, 1999).
Physical readiness is of
vital importance, because until a per-son is physically capable of learning,
attempts at teaching and learning may be both futile and frustrating. For
example, some-one in acute pain will be unable to focus attention away from the
pain long enough to concentrate on learning. Likewise, a person who is short of
breath will concentrate on breathing rather than on learning.
Emotional readiness also affects the motivation to learn. A person who has not accepted an existing illness or the threat of illness will not be motivated to learn. People who do not accept a therapeutic regimen, or who view it as conflicting with their present lifestyle, may consciously avoid learning about it.
Until a person recognizes the
need to learn and demonstrates an ability to learn, teaching efforts may be
thwarted. However, it is not al-ways wise to wait for a patient to become
emotionally ready to learn, because that time might never come unless efforts
are made by the nurse to stimulate the individual’s motivation.
Illness and the threat
of illness are usually accompanied by anxiety and stress. The nurse who
recognizes such reactions can use simple explanations and instructions to
alleviate these anxi-eties and provide further motivation to learn. Because
learning involves changes in behavior, it normally produces mild anxiety, which
can often be a useful motivating factor.
Emotional readiness can
be promoted by creating a warm, ac-cepting, positive atmosphere and by
establishing realistic learning goals. When learners achieve success and a
feeling of accomplish-ment, they experience further motivation for
participating in additional learning opportunities.
Feedback about progress also motivates learning. Such
feed-back should be presented in the form of positive reinforcement when
learners are successful and in the form of constructive sug-gestions for
improvement when they are unsuccessful.
Experiential readiness
refers to past experiences that influence a person’s ability to learn. Previous
educational experiences and life experiences in general are significant
determinants of an in-dividual’s approach to learning. A person who has had
little or no formal education may not be able to understand the instructional
materials presented. A person who has had difficulty learning in the past may
be hesitant to try again. Many behaviors required for reaching maximum health
potential demand a rather exten-sive background of knowledge, physical skills,
and attitudes. With-out this background on which to build, learning may be very
difficult and very slow. For example, someone who does not under-stand the
basics of normal nutrition may not be able to under-stand the restrictions of a
specific diet. A person who does not view the desired learning as personally
meaningful may reject teaching efforts. A person who is not future-oriented may
be un-able to appreciate many aspects of preventive health teaching.
Experiential readiness is closely related to emotional readiness because
motivation tends to be stimulated by an appreciation for the need to learn and
by those learning tasks that are familiar, in-teresting, and meaningful.
Before initiating a
teaching–learning program, it is important to assess the learner’s physical and
emotional readiness to learn, as well as his or her ability to learn what is
being taught. This in-formation then becomes the basis for establishing goals
that can motivate the person to learn. Involving the learner in the
estab-lishment of mutually acceptable goals serves the purpose of en-couraging
active involvement in the learning process and a willingness to share the
responsibility for learning.
THE LEARNING ENVIRONMENT
Although learning can
take place without a teacher, most people who are attempting to learn new or
altered health behaviors will need the services of a nurse for at least part of
the time. The in-terpersonal interaction between the learner and the nurse who
is attempting to meet the individual’s learning needs may be formal or
informal, depending on the method and techniques of teach-ing that are found to
be most appropriate.
Learning can be
optimized by minimizing external variables that interfere with the learning
process. For example, the room temperature, lighting, noise levels, and other
environmental con-ditions should be appropriate to the learning situation.
Also, the time selected for teaching should be suited to the individual’sneeds.
Scheduling a teaching session at a time of day when the pa-tient is fatigued, uncomfortable,
or anxious about a pending di-agnostic or therapeutic procedure, or when
visitors are present, does not provide an environment conducive to learning.
How-ever, if family members are to participate in providing care, the sessions
should be timed to take place when the family is present so that they can learn
any necessary skills or techniques.
TEACHING TECHNIQUES
Teaching techniques and
methods enhance learning if they are appropriate to the individual’s needs.
Numerous techniques are available, including lectures, group teaching, and
demonstra-tions, all of which can be enhanced with specially prepared teach-ing
materials. The lecture or explanation method of teaching is commonly used but
should always be accompanied by discussion. Discussion is important because it
affords the learner an oppor-tunity to express feelings and concerns, to ask
questions, and to receive clarification.
Group teaching is
appropriate for some people because it al-lows them not only to receive needed
information, but also to feel secure as members of a group. Those with similar
problems or learning needs have the opportunity to identify with each other and
gain moral support and encouragement. However, not every-one relates or learns
well in groups, and some people may not benefit from such experiences. Also, if
group teaching is used, as-sessment and follow-up of each individual are
imperative to en-sure that each has gained sufficient knowledge and skills.
Demonstration and
practice are essential ingredients of a teaching program, especially when
teaching skills. It is best to demonstrate the skill and then allow the learner
ample opportu-nity for practice. When special equipment is involved, such as
syringes for injections, colostomy bags, dialysis equipment, dress-ings, or
suction apparatus, it is important to teach with the same equipment that will
be used in the home setting. Learning to per-form a skill with one kind of
equipment and then having to change to a different kind may lead to confusion,
frustration, and mistakes.
Teaching aids that are
available to enhance learning include books, pamphlets, pictures, films,
slides, audio and video tapes, models, programmed instruction, and
computer-assisted learn-ing modules. Such teaching aids are invaluable when used
ap-propriately and can save a significant amount of personnel time and related
cost. However, all such aids should be reviewed be-fore use to ensure that they
meet the individual’s learning needs. Human interaction and discussion cannot
be replaced by teach-ing technologies but may be enhanced by them (Nursing
Research Profile 4-1).
Reinforcement and
follow-up are important because learning takes time. Allowing ample time to
learn and reinforcing what is learned are important teaching strategies; a single
teaching session is rarely adequate. Follow-up sessions are imperative to
promote learners’ confidence in their abilities and to plan for additional
teaching sessions. For hospitalized patients who may not be able to transfer
what they have learned in the hospital to the home set-ting, follow-up after
discharge is essential to ensure that they have realized the full benefits of a
teaching program.
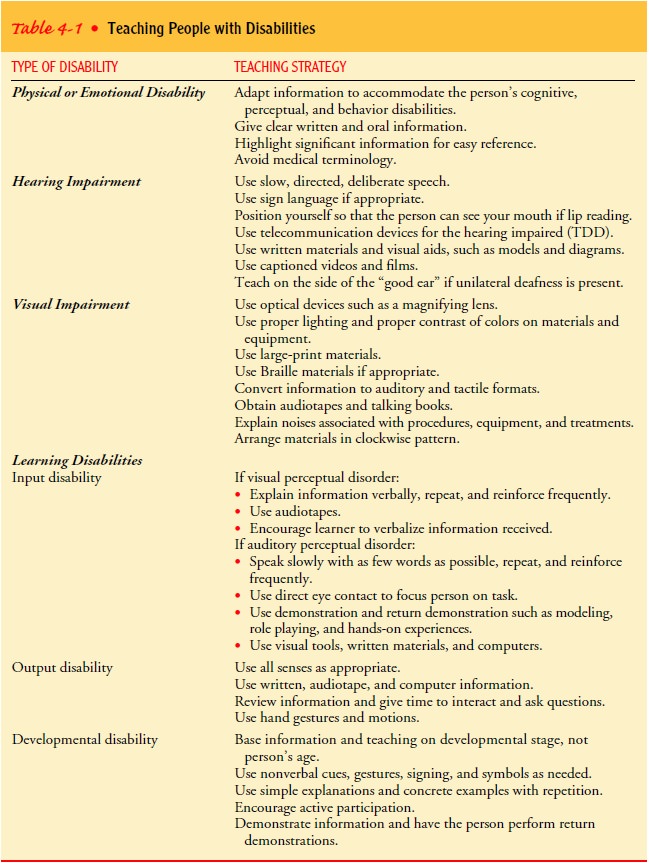
TEACHING PEOPLE WITH DISABILITIES
When providing health
information to people who are affected by disabilities, the individual needs of
the person must be assessed and incorporated into the teaching plan; teaching
techniques and
GERONTOLOGIC CONSIDERATIONS
Nurses caring for elderly people must be aware of how the nor-mal changes that occur with aging affect learning abilities and how an elderly person can be assisted to adjust to these changes. Above all, it is important to recognize that just because a person is elderly does not mean that he or she cannot learn. Studies have shown that older adults can learn and remember if information is paced appropriately, is relevant, and is followed by appropri-ate feedback strategies that apply to all learners (Rankin & Stallings, 2000). Because changes associated with aging vary significantly among elderly people, the nurse should conduct a thorough assessment of each person’s level of physiologic and psychological functioning before teaching begins.
Changes in cognition
with age may include slowed mental functioning; decreased short-term memory,
abstract thinking, and concentration; and slowed reaction time. These changes
are often accentuated by the health problems that cause the el-derly to seek
health care in the first place. Effective teaching strategies include a
slow-paced presentation of small amounts of material at a time, frequent
repetition of information, and the use of reinforcement techniques, such as
audiovisual and written materials and repeated practice sessions. Distracting
stimuli should be minimized as much as possible in the teach-ing environment.
Sensory changes
associated with aging also affect teaching and learning. Teaching strategies to
accommodate decreased visual acuity include large-print and easy-to-read
materials printed on non-glare paper. Because color discrimination is often
impaired, the use of color-coded or highlighted teaching materials may not be
effective. To maximize hearing, the teacher must speak dis-tinctly with a
normal or lowered pitch, facing the person so that lip reading can occur as needed.
Visual cues often help to rein-force verbal teaching.
Family members should be
involved in teaching sessions when possible. They provide another source for
reinforcement of ma-terial and can help the learner to recall instructions
later. They can also provide valuable assessment information about the
per-son’s living situation and related learning needs.
When the nurse, the
family, and other involved health care professionals work collaboratively to
facilitate an elderly person’s learning, the chances of success will be
maximized. Successful learning for the elderly should result in improved
self-care man-agement skills, enhanced self-esteem, and a willingness to learn
in future sessions.
Related Topics